Official Newsjournal of the Illinois Council of Health-System Pharmacists

November 2021
Volume 47 Issue 4
Features
Call for Entries: 2017 Best Practice Award
Columns
Educational Affairs Poster Abstracts
College Connection
Developing Leadership, A Reflection
More
ICHP Pharmacy Action Fund (PAC) Contributors
Officers and Board of Directors
KeePosted Info
Loves Park, IL 61111-8653
Phone: (815) 227-9292
Fax: (815) 227-9294
ichpnet.org
KeePosted
Official Newsjournal of the Illinois Council of Health-System Pharmacists
EDITOR
Jacob Gettig
ASSISTANT EDITOR
Jennifer Phillips
MANAGING EDITOR
Scott Meyers
ASSISTANT MANAGING EDITOR
Trish Wegner
DESIGN EDITOR
Leann Nelson
EXECUTIVE VICE PRESIDENT
Scott Meyers
VICE PRESIDENT - PROFESSIONAL SERVICES
Trish Wegner
DIRECTOR OF OPERATIONS
Maggie Allen
INFORMATION SPECIALIST
Heidi Sunday
CUSTOMER SERVICE AND
PHARMACY TECH TOPICS™ SPECIALIST
Jo Ann Haley
ACCOUNTANTS
Jan Mark and Trisha Blassage
COMMUNICATIONS MANAGER
Leann Nelson
ICHP Mission Statement
Advancing Excellence in Pharmacy
ICHP Vision Statement
ICHP dedicates itself to achieving a vision of pharmacy practice where:
- Pharmacists are universally recognized as health care professionals and essential providers of health care services.
- Patients are aware of the training, skills, and abilities of a pharmacist and the fundamental role that pharmacists play in optimizing medication therapy.
- Formally educated, appropriately trained, and PTCB certified pharmacy technicians manage the medication distribution process with appropriate pharmacist oversight.
- Pharmacists improve patient care and medication safety through the development of effective public policies by interacting and collaborating with patients, other health care professionals and their respective professional societies, government agencies, employers and other concerned parties.
- Evidence-based practices are used to achieve safe and effective medication therapies.
- There are an adequate number of qualified pharmacy leaders within the pharmacy profession.
- Pharmacists take primary responsibility for educating pharmacy technicians, pharmacy students, pharmacist peers, other health professionals, and patients about appropriate medication use.
KeePosted Vision
As an integral publication of the Illinois Council of Health-System Pharmacists, the KeePosted newsjournal will reflect its mission and goals. In conjunction with those goals, KeePosted will provide timely information that meets the changing professional and personal needs of Illinois pharmacists and technicians, and maintain high publication standards.
KeePosted is an official publication of, and is copyrighted by, the Illinois Council of Health-System Pharmacists (ICHP). KeePosted is published 10 times a year. ICHP members received KeePosted as a member benefit. All articles published herein represent the opinions of the authors and do not reflect the policy of the ICHP or the authors’ institutions unless specified. Advertising inquiries can be directed to ICHP office at the address listed above. Image disclaimer: The image used in the Pharmacy Tech Topics™ advertisement is the property of © 2017 Thinkstock, a division of Getty Images.
Copyright © 2017, Illinois Council of Health-System Pharmacists. All rights reserved.
Features
Ambulatory Care Network
Help Us Help You (to Advance Pharmacy Practice)
Feature Article
by Brian T. Cryder, PharmD BCACP CACP, Associate Professor of Pharmacy Practice; Reggie Greenwood, Midwestern University Chicago College of Pharmacy Candidate Class of 2019, Phi Delta Chi - Beta Xi, Professionalism Committee Chair
Call for Entries: 2017 Best Practice Award
Feature Article

- Innovativeness / originality
- Contribution to improving patient care
- Contribution to institution and pharmacy practice
- Scope of project
- Quality of submission
Previous Winners
http://ichpnet.org/pharmacy_practice/professional_practice/best_practices/application_form/
- Introduction, Purpose, and Goals of the program
- Description of the program
- Experience with and outcomes of the program
- Discussion of innovative aspects of programs and achievement of goals
- Conclusion
- The program will be featured at the ICHP Annual Meeting. You will need to prepare a poster to present your program and/or give a verbal presentation. Guidelines will be sent to the winner.
- You will be asked to electronically submit your manuscript to the ICHP KeePosted for publishing. This program will be accredited for CPE and will require that you complete material for ACPE accreditation.
- You will receive a complimentary registration to the ICHP Annual Meeting, recognition at the meeting and a monetary award distributed to your institution.
- Non-winning submissions may also be considered for publication in the ICHP KeePosted, but your permission will be obtained beforehand.
Columns
 President's Message
President's Message
Which Came First: Innovation or Collaboration? Part 2 of 2
by Charlene Hope, PharmD, MS, BCPS, ICHP President
- Not having enough time to invite feedback from others
- The practical difficulty of having too many ideas to manage
- Greater risk of conflict amongst stakeholders
- A fear of losing control of the project’s direction
- If you don’t have regular staff meetings then start— bi-weekly, weekly, monthly — that allow each team member to have a voice. Ask questions and send an outline before each meeting that goes over expectations. Allow time for each individual to share and discuss recent on-goings in and outside of the pharmacy..
- Remember the team building activities you did in school? Why not take them to the next level in the pharmacy. Create quarterly events that take employees out of the office — think walks, bowling, museum tours, dinner cruises, plain dinners — the options are endless.
- Solidify your on-boarding process by making proper introductions a priority. Introduce new employees and team members.
- Make inter-team introductions when you see a lack of communication. Encourage meetings among “Peas in a pod” various departments and make introductions based on innovative potential.
 Directly Speaking
Directly Speaking
What Keeps You Up at Night?
by Scott A. Meyers, Executive Vice President
I suspect, from personal experience, that anyone’s answer if that question is asked will depend on which time of year it is, which night of the week it is or even how old you are. I assume it happens to many if not all of you but the frequency and duration probably vary based on age and level of responsibility at home and at work.
So what keeps you, our members up at night, and is there something we can do to help you deal with it? If the answer is money, probably not. Although our dues are very reasonable and lag far behind many other pharmacy and health care professional organizations in Illinois and across the nation. And our meetings are a bargain! If you’ve attended a recent Midyear or APhA Annual Meeting, you know exactly what I mean. I personally, am contemplating attending an association executive meeting in August, and the registration fee for that is $899!
If what keeps you up at night is pharmacy practice related, we can help. In addition to the cutting-edge education that our Educational Affairs Division provides through the Champion webinars and CPRN (Clinical Practice and Research Network) programs and what the Meeting Planning Committees produce for the Spring and Annual Meetings, ICHP provides a variety of opportunities to network with your peers at meetings and online.
If it’s not money or practice related problems, what about the expansion of practice or practicing at the top of your license? ICHP’s Division of Government Affairs works year-in and year-out to guide legislation and regulation that will create a scope of pharmacy practice that matches where today’s education is aiming. Unfortunately, it doesn’t mean we’re there yet, but every day that group is pushing closer and closer to where we need to be.
Drug pricing has been keeping me from getting my rest lately. As I see new products that come to market with costs of more than a year’s salary for any pharmacist, let alone someone near the poverty level, I question when and where it will all end? It looks like it could be soon as Congress and the General Assembly begin taking up drug pricing legislation as a result of these outrageous prices!
I also lose sleep over the way health care and pharmacy specifically are paid! PBM’s seem to have lost their cost-savings focus and crossed over to the dark-side, snagging profits and savings for themselves with much of it coming from the backs of their pharmacist colleagues in the community practice settings! Initially, PBM’s did a great job of saving employers money on the medication side of the insurance equation. But now as they cut themselves in for more and more of the rebates they collect while slicing dispensing fees and medication cost reimbursements down to nearly nothing, the pharmacists who run these PBM’s have forgotten what value a pharmacist could bring if they would only pay them for their MTM services!
Most importantly to me is the cost of health care! Whether the Republicans in Congress are successful in repealing and replacing the Affordable Care Act doesn’t keep me up at night. Hoping that all of Congress realizes, soon enough, that the entire system is broken and needs more than a simple plan switch, does! Health care is a benefit every human should receive, at least at a basic level. And our nation should be able to provide a basic system that provides care as well as any in the world.
But every human needs to respect and value that benefit by doing everything in their power to help their own outcomes. This means eating well balanced healthy meals, exercising, adhering to medication and other therapies, not smoking, and avoiding other risky behaviors. It also means using the system correctly. Finding a primary care physician or other provider and not using the emergency rooms for non-emergencies. Unfortunately, I’m not sure what you do with those who continue to disrespect and misuse the system? But wouldn’t it be nice if that was our biggest health care problem?
It also means we will all have to pay for it – which many individuals will protest. I’m sure we’ll hear, “Why do I have to pay for someone’s pregnancy when I’m a 60-year old guy?” But this 60+ year old guy understands why that’s necessary. Or we’ll hear from the younger generation, “I’m healthy, why do I need to pay for some old guy’s health care?” If they’re lucky and live right, they will become that old guy or gal! So none of that will keep me up at night. Perhaps it’s time to admit that everyone will need to pay for health care for everyone. Just like we pay for retirement for everyone. One less thing to keep us up.
There are plenty of problems to keep every American up at night, but I’m not sure it’s happening enough. If it were, we would probably be closer to a reasonable solution. If that ever happens with health care, we can shift gears and spend our sleeplessness worrying about global warming, running out of fossil fuels or the day that giant asteroid eventually changes life on earth as we know it! I’m sorry if I have given you more to keep you up at night, but maybe if we all spent a few more sleepless minutes thinking about it, somebody will actually do something positive about it!
ICHPeople
Congratulations Elizabeth Wozniak on the birth of her daughter: Cora Elizabeth! 
This is Cora Elizabeth Wozniak. She was born on 3/2/17 at 7 pounds, 3 ounces and 21 inches long.
____________________________________________________
Two ICHP Past Presidents receive ASHP Honors! Two more ICHP members become Fellows of ASHP!
Max L. (Mick) Hunt, R.Ph., M.S., M.B.A., FASHP, Associate Professor Emeritus, College of Pharmacy, Northeast Ohio Medical University, Rootstown, Ohio and ICHP Past President (1979-1980) has been named this year’s recipient of ASHP’s Harvey A. K. Whitney Award, ASHP’s highest honor.
Mr. Hunt is a pharmacy leader with a long career in pharmacy
administration and education who is noted for his role in the adoption of key
advancements in pharmacy practice, commitment to developing future generations
of pharmacy leaders, and active service to the profession. Mick will receive his award and make his
Whitney Lecture Presentation at the ASHP Summer Meeting in Minneapolis in June.
Read more here: https://www.ashp.org/news/2017/03/09/20/39/hunt-to-receive-2017-whitney-award

Caryn Dellamorte Bing, R.Ph., M.S., FASHP, Principal Consultant, CB Healthcare Consulting, Las Vegas and ICHP Past President (1987-1988) will receive ASHP’s 2017 Distinguished Leadership Award for Ambulatory Care at the ASHP Midyear Meeting in Orlando, Florida in December.
Ms. Bing is a nationally recognized expert, author, and speaker with more than 35 years of practice and management experience in home care, specialty, and acute care pharmacy.
ICHP members Jan Keresztes and Jennifer Phillips (ICHP Past President 2016-2017) have also been named Fellows of the American Society of Health-System Pharma
cists and will receive their Fellow recognition at the 2017 ASHP Summer Meeting in Minneapolis in June.
Congratulations to all of these outstanding pharmacy leaders and current and former ICHP members! Congratulate them on the ICHP Facebook page here on our Facebook POST.
___________________________________________________________
ICHP Welcomes New Communications Manager, Leann Nelson
 Hello I am your new Communications Manager for ICHP. I
started in the position on February 9th and hit the ground running
with an issue of KeePosted and Pharmacy Tech Topics™
due shortly after my arrival!
Hello I am your new Communications Manager for ICHP. I
started in the position on February 9th and hit the ground running
with an issue of KeePosted and Pharmacy Tech Topics™
due shortly after my arrival!
You may have seen me travelling with a group of students on Legislative Day 2017 snapping photos under the dome as well as at the ICHP/MSHP Spring Meeting March 30 - April 1. I was honored to be a part of these exciting events!
My professional experience includes 16 years in graphic design, event planning, and communications in the real estate industry as marketing coordinator and social media specialist for the area’s largest broker. In addition, I worked briefly as a property manager and marketing associate for a local builder. I left the real estate industry and spent a few years as an executive administrative assistant, board secretary and IT manager for the AHL Rockford IceHogs at the arena in downtown Rockford.
I am a life-long resident of the Rockford, IL area and mother to one teenage boy. We have two adopted dogs. My son and I enjoy attending local concerts, bowling, dining out and trips to Chicago to see the Blackhawks play. During my free time, I like to sing karaoke as well as volunteer as an adult mentor for young ladies in a local recovery home.
I am learning a great deal in my first weeks here and look forward to the challenges of this new position. I plan to put my talent and experience to good use for ICHP and all of its members. Connect with me here: https://www.linkedin.com/in/leannnelson or email me anytime at lnelson@ichpnet.org.
Hi-Tech
How I Joined the Pharmacy Technician Profession
by Clara Gary, Pharmacy Technician
Government Affairs Report
HB2392 is Not the Fix We Need
by Jim Owen and Scott Meyers
This is the first time in many years that we have actually received pushback from our members on a legislative issue – which is actually a good thing from the perspective that some of our members are paying attention to what goes on in Springfield. And we realize it’s our job to really pay attention to what goes on in Springfield, so we would like to share some of the details that you, our members, don’t have time to see.
First,
let us describe what the real HB2392 does and doesn’t do for pharmacy:
- The bill would set a prescription filling limit of 10 prescriptions per hour in a pharmacy.
- It would require at least one pharmacy technician to be on duty whenever the practice of pharmacy is conducted.
- It would mandate two 15-minute breaks and a 30-minute meal for every pharmacist who works at least 7 hours.
- If a pharmacist has to work during their lunch or break period, the pharmacy is required to pay that pharmacist triple time for the entire day.
- It would prohibit employers from requiring pharmacists to participate in activities such as advertising or soliciting that may jeopardize patient health, safety or welfare or any activities or external factors, including promotional requirements and productivity quotas that interfere with the pharmacist’s ability to provide appropriate professional services.
- The bill would require pharmacies to prohibit their pharmacists from working more than an 8-hour shift.
- It would require every pharmacy “to make available at all times a room on the pharmacy’s premises with adequate seating and tables for the purpose of allowing the pharmacist to enjoy break periods in a clean and comfortable environment”. This is the exact language from this bill!
- The pharmacy would be required to keep a complete and accurate record of the break periods of its pharmacists.
- The bill requires every pharmacy to keep records of any errors in the receiving, filling, or dispensing of prescriptions of any kind, including any errors resulting in an adverse drug interaction or adversely affecting the health of the patient.
- The bill does provide whistleblower protection to any pharmacy employee that reports violations of the Act.
Hopefully, it is crystal clear that this bill is flawed! Very flawed. As it is currently written, this bill would hamstring pharmacies and slow the processing of prescription orders so that within a week, most pharmacies would be behind by at least another week. Even if the language is rewritten so that the 10 prescription per hour limit is per pharmacist rather than pharmacy, there would need to be a dramatic demand for additional pharmacists creating significant cost increases for every pharmacy, unless that is, they cut pharmacist wages by one-half or more! And since there is a significant surplus of pharmacists, that might be the answer. One answer we’re sure our members won’t support.
But even more critical, this bill prevents pharmacies from using 7-on-7-off scheduling for third shifts and four 10-hour day scheduling at any time! Do we really want that? I think it will become exceedingly hard to staff 24-hour pharmacies anywhere if shifts are mandated to be 8-hours or less.
The error reporting language is catastrophic – every single error in receiving, filling or dispensing! That means even if there is no impact on the patient. That means errors made by technicians and caught by pharmacists or other technicians would need to be written up and retained for 5 years. It will be very easy for a plaintiff’s lawyer to establish a pattern of errors or negligence with these records available and unprotected.
Yes, the mandated lunch is reasonable and yes, the whistleblower protection is acceptable. But those limited benefits don’t come close to outweighing the damage this bill would do to pharmacies and their staffs in general. ICHP is fighting this bill because of the shift restrictions and orders per hour limit. We do not support the tactics that some chain employers use to measure productivity and performance.
ICHP has been questioned about our relationship with the Illinois Retail Merchants Association (IRMA) who represent the chain pharmacies. Why we aren’t sympathetic to the plight of our colleagues in the chains – the colleagues who claim to get no bathroom or meal breaks. Truthfully, we are sympathetic to the rank and file chain employee. But the situation is Springfield demands something most pharmacists don’t understand.
Springfield demands a unified front from pharmacy if we are to be taken seriously. If ICHP says one thing, IPhA another and IRMA yet another, the General Assembly and the various agencies walk away. They listen to the biggest voices in Springfield and pharmacy unified is still small but worth listening to, however, separately, even IRMA’s credibility is questioned. So many times we hear, “How does the pharmacists’ association feel about this bill?” and “what about IRMA?” If a legislator hears something different from anyone of us, their immediate response is, “Come back and talk to us when pharmacy can get its position together!”
Is that fair? Of course not. Every interested party should be heard. But in Springfield the pharmacy vote is relatively small compared to many industries, so fractured positions carry even less weight. Therefore, it is critical when a bill comes along that none of us like, we fight it together, regardless of the different reasons for not liking it.
So now collectively, ICHP, IPhA and IRMA are fighting a bill that is bad for pharmacy practice and our patients, but through this fight makes each of us look like we don’t care about our colleagues in the profession. That couldn’t be further from the truth. What is true is that all three organizations have lost faith in those pharmacists whose continued mantra is “I don’t have time to counsel the patient!” In a subject matter hearing on February 22nd, Rep. Mary Flowers blamed the employers for creating that attitude because “pharmacists work for two masters and the primary master is their employer.” I (Scott) told her that every pharmacist takes an oath at graduation, to serve their patients first, with these very words, “I will consider the welfare of humanity and relief of suffering my primary concerns.” Those pharmacists who failed to counsel their patients let those patients down, let their community down and let their profession down. And now because they failed to serve their primary concerns, we fight this horrible bill together.
ICHP is now monitoring over 80 bills and resolutions in the 100th General Assembly, and this list is provided for your review. For more details on the bills or resolutions that have significant impact on pharmacy, go to www.ilga.gov and click on the tab titled “Bills and Resolutions”. Some bills are not included below as they are shell bills or fringe bills that we monitor but do not feel currently warrant concern.
2017 Illinois General Assembly Bill Summary
|
Bill Number |
Sponsor |
Summary |
Location |
ICHP Position |
|
SB0073 HB0239 |
Silverstein – Chicago, D |
Amends the Illinois Food, Drug and Cosmetic Act. Adds provision concerning prescription drug price increases. Requires manufacturers of prescription drugs to notify State purchasers, health insurers, health care service plan providers, and pharmacy benefit managers of specified increases in drug prices at least 30 days before such increase and the cost of specified new prescription drugs 3 days before the commercial availability of a new drug approved by the U.S. Food and Drug Administration or within 3 days after approval by the U.S. Food and Drug Administration if the new drug will be made commercially available within 3 days of such approval. Provides that within 30 days after such notifications, prescription drug manufacturers shall report specified information to the Department of Public Health and requires the Department to publish such information on its website. Provides that failure to report such information to specified entities shall result in a specified administrative penalty. Provides that the Department may adopt rules and issue guidance to implement these provisions and shall be responsible for enforcing these provisions. Contains provisions concerning the confidentiality of pricing information. Repeals provisions concerning prescription drug price increases on January 1, 2022. Effective immediately. |
Human Services Comm. |
|
|
SB0625 |
Martinez – Chicago, D |
Amends the Regulatory Sunset Act. Extends the repeal of the Nurse Practice Act from January 1, 2018 to January 1, 2028. Amends the Nurse Practice Act. Defines "focused assessment", "full practice authority", "oversight", and "postgraduate advanced practice nurse". Changes references of "advanced practice nurse" and "APN" to "advanced practice registered nurse" and "APRN" throughout the Act. Replaces provisions regarding nursing delegation with provisions that prohibit specified actions. Provides other guidelines for delegation of nursing activities and medication administration. Makes changes to education program requirements, qualifications for licensure, the scope of practice, and continuing education for LPN and RN licensees. Provides that a written collaborative agreement is required for all postgraduate advanced practice registered nurses until specific requirements have been met. Provides that postgraduate advanced practice registered nurses may enter into written collaborative agreements with collaborating advanced practice registered nurses or physicians (rather than collaborating physicians or podiatric physicians). In provisions concerning prescriptive authority for postgraduate advanced practice registered nurses, sets forth the requirements for postgraduate advanced practice registered nurses to have prescriptive authority and the limitations of such authority. Makes changes to provisions concerning the grounds for disciplinary action under the Act. Requires the Department of Public Health to prepare a report regarding the moneys appropriated from the Nursing Dedicated and Professional Fund to the Department of Public Health for nursing scholarships. Makes other changes. Effective immediately. |
Licensed Activities and Pensions Comm. |
Oppose |
|
SB0636 |
Link – Gurnee, D |
Amends the Pharmacy Practice Act. Provides that the Act shall not apply to, or in any manner interfere with, the sale or distribution of dialysate, drugs, or devices necessary to perform home renal dialysis for patients with chronic kidney failure, provided that certain conditions are met. Effective immediately. |
Amended on 2nd Reading in the Senate |
|
|
SB0642 |
Steans – Steans, D |
Amends the Nurse Practice Act. In provisions concerning scope of practice, written collaborative agreements, temporary practice with a collaborative agreement, prescriptive authority with a collaborative agreement, titles, advertising, continuing education, and reports relating to professional conduct and capacity, changes references of "advanced practice nurse" and "APN" to "advanced practice registered nurse" and "APRN". Provides that a written collaborative agreement is required for all postgraduate advanced practice registered nurses until specific requirements have been met. Provides that postgraduate advanced practice registered nurses may enter into written collaborative agreements with collaborating advanced practice registered nurses or physicians (rather than collaborating physicians or podiatric physicians). In provisions concerning prescriptive authority for postgraduate advanced practice registered nurses, sets forth the requirements for postgraduate advanced practice registered nurses to have prescriptive authority and the limitations of such authority. Defines "full practice authority" and provides requirements for it to be granted to an advanced practice registered nurse. Removes provisions concerning advanced practice nursing in hospitals, hospital affiliates, or ambulatory surgical treatment centers, except the provision for anesthesia services and the provision requiring advanced practice registered nurses to provide services in accordance with other Acts. Makes other changes. Effective immediately. |
2nd Reading in the Senate. |
Oppose |
|
SB0680 |
Althoff – McHenry, R |
Amends the Safe Pharmaceutical Disposal Act. Provides that used, expired, or unwanted pharmaceuticals collected by a city, village, or municipality under the Act may be destroyed in a drug destruction device by a law enforcement agency. Amends the Environmental Protection Act. Expands the definition of "drug evidence" in the provision for drug destruction by a law enforcement agency to include any used, expired, or unwanted pharmaceuticals collected under the Safe Pharmaceutical Disposal Act. |
2nd Reading in the Senate. |
|
|
SB0892 |
Tracy – Quincy, R |
Amends the Illinois Controlled Substances Act. Provides that the Department of Human Services may release information received by the central repository to select representatives of the Department of Children and Family Services through the indirect online request process. Provides that access shall be established by the Prescription Monitoring Program Advisory Committee by rule. |
Human Services Comm. |
|
|
SB0900 |
Althoff – McHenry, R |
Amends the Regulatory Sunset Act. Extends the repeal date of the Nurse Practice Act from January 1, 2018 to January 1, 2028. Amends the Nurse Practice Act. Eliminates the position of Assistant Nursing Coordinator. Eliminates the Advanced Practice Nursing Board. Provides that the Department of Financial and Professional Regulation may provide notice to a licensee or applicant by certified or registered mail to the address of record or by email to the email address of record. Provides provisions for change of address of record and email address of record, application for license, confidentiality of any information collected by the Department in the course of an examination or investigation of a license or applicant, and disposition by a consent order. Changes references to "advanced practice nurse" to references to "advanced practice registered nurse" throughout the Act and other Acts. Changes references to "Illinois Center for Nursing" to references to "Illinois Nursing Workforce Center". Makes changes concerning definitions, application of the Act, unlicensed practice, prohibited acts, Department powers and duties, nursing delegation, qualifications for LPN, RN, and APRN licensure, RN education program requirements, grounds for disciplinary action, intoxication and drug abuse, the Nursing Dedicated and Professional Fund, investigations, notices, hearings, use of stenographers and transcripts, review under the Administrative Review Law, certification of records, the Center for Nursing Advisory Board, and medication aide licensure requirements. Removes provisions concerning registered nurse externship permits, rosters, liability of the State, hearing officers, and orders for rehearings. Makes other changes. Effective immediately. |
Licensed Activities and Pensions Comm. |
|
|
SB0902 same as HB3462 |
Righter – Mattoon, R |
Amends the Regulatory Sunset Act. Extends the repeal date of the Pharmacy Practice Act from January 1, 2018 to January 1, 2028. Amends the Pharmacy Practice Act. Provides that all applicants and licensees shall provide a valid address and email address, which shall serve as the address and email address of record, and shall inform the Department of Financial and Professional Regulation of any change of address or email address through specified means. Provides for the licensure (rather than registration) of registered pharmacy technicians, registered certified pharmacy technicians, and pharmacists, and makes conforming changes. Removes provision allowing each member of the State Board of Pharmacy to receive a per diem payment in an amount determined from time to time by the Secretary of Financial and Professional Regulation for attendance at meetings of the Board and conducting other official business of the Board. Changes references to "Director" to references to "Secretary" or "Department" throughout the Act. Eliminates the position of deputy pharmacy coordinator. Makes changes in provisions concerning definitions, duties of the Department, inactive status, pharmacists in charge, nonresident pharmacy licenses, record retention, automated pharmacy systems, remote prescription processing, and discipline. Makes other changes. Effective immediately. |
Licensed Activities and Pensions Comm. |
|
|
SB1546 same as HB2957 |
Mulroe – Chicago, D |
Amends the Illinois Insurance Code. Provides that every policy of accident and health insurance amended, delivered, issued, or renewed after the effective date of the amendatory Act that provides coverage for prescription drugs shall provide for synchronization of prescription drug refills on at least one occasion per insured per year provided that certain conditions are met. Requires insurers to provide prorated daily cost-sharing rates when necessary. Makes conforming changes in the State Employees Group Insurance Act of 1971, the Counties Code, the Illinois Municipal Code, the School Code, the Health Maintenance Organization Act, the Limited Health Services Organization Act, the Voluntary Health Services Plan Act, and the Illinois Public Aid Code. Effective immediately. |
2nd Reading in the Senate |
|
|
SB1596 same as HB2908 |
Righter - Mattoon, R |
Amends the Medical Assistance Article of the Illinois Public Aid Code. In provisions concerning medical assistance for the treatment of alcohol dependence or opioid dependence, provides that on or after July 1, 2017 such coverage may be subject to utilization controls or prior authorization mandates consistent with the most current edition of the American Society of Addiction Medicine's National Practice Guideline for the Use of Medications in the Treatment of Addiction Involving Opioid Use, as now or hereafter revised, or any successor publication (rather than on or after July 1, 2015 such coverage shall not be subject to any (1) utilization control, other than those established under the American Society of Addiction Medicine patient placement criteria, (2) prior authorization mandate, or (3) lifetime restriction limit mandate). Provides that on or after July 1, 2017, opioid antagonists prescribed for the treatment of an opioid overdose may be subject to (A) utilization controls or (B) prior authorization mandates consistent with the most current edition of the American Society of Addiction Medicine's National Practice Guideline for the Use of Medications in the Treatment of Addiction Involving Opioid Use, as now or hereafter revised, or any successor publication. |
Human Services Comm. |
|
|
SB1604 |
Nybo – Lombard, R |
Amends the Pharmacy Practice Act. Provides that if a physician or other authorized prescriber does not prohibit drug product substitution, a pharmacist shall dispense a brand name drug product as a substitute for an unavailable nonbrand name drug product specified in the prescription. Provides that if the substitute drug product has a unit price greater than the unavailable drug product specified in the prescription, then the pharmacist shall dispense that substitute drug product at the lesser unit price of the drug product specified in the prescription. Amends the Regulatory Sunset Act to extend the repeal date for the Pharmacy Practice Act to January 1, 2020. Makes conforming changes. Effective immediately. |
Licensed Activities and Pensions Comm. |
Oppose |
|
SB1607 |
Bush – Grayslake, D |
Amends the Illinois Controlled Substances Act. Requires prescribers to check PMP prior to writing any prescriptions of CII, III, IV, or V medications. Requires prescriber to note knowledge of a report received on specific patient from DHS. Requires pharmacists to review PMP if they know of an individual who is the subject of a report by DHS. The pharmacy or pharmacist must contact the prescriber and obtain a signature of acknowledgement before dispensing. Requires DHS to write rules within one year that requires all electronic medical records to interface with the PMP by Jan. 1, 2021. |
Licensed Activities and Pensions Comm. |
|
|
SB1609 same as HB2956 |
Bush – Grayslake, D |
Amends the Illinois Insurance Code, the State Employees Group Insurance Act of 1971, the Counties Code, the Illinois Municipal Code, the School Code, the Health Maintenance Organization Act, the Limited Health Service Organization Act, the Voluntary Health Services Plans Act, and the Illinois Public Aid Code. Prohibits insurers from requiring that a covered individual first use an opioid analgesic drug product without abuse-deterrence labeling claims before providing coverage for an abuse-deterrent opioid analgesic drug product. |
Insurance Comm. |
|
|
SB1660 Same as HB2892 |
McCarter – Vandalia, R |
Amends the Workers' Compensation Act. Provides that no medical provider shall be reimbursed for a supply of prescriptions filled outside of a licensed pharmacy except when there exists no licensed pharmacy within 5 miles of the prescribing physician's practice. Provides that, if there exists no licensed pharmacy within 5 miles of the prescribing physician's practice, no medical provider shall be reimbursed for a prescription, the supply of which lasts for longer than 72 hours from the date of injury or 24 hours from the date of first referral to the medical service provider, whichever is greater, filled and dispensed outside of a licensed pharmacy. Provides that the limitations on filling and dispensing prescriptions do not apply if there exists a pre-arranged agreement between the medical provider and a preferred provider program regarding the filling of prescriptions outside a licensed pharmacy. |
Subcomm. On Tort Reform |
|
|
SB1790 |
Stadelman – Rockford, D |
Amends the Pharmacy Practice Act. Provides that a pharmacist may refill a patient's prescription without prescriber authorization if the pharmacist is unable to contact the prescriber after reasonable effort, a failure to refill the prescription may result in an interruption of therapeutic regimen or create patient suffering, the pharmacist informs the prescriber at the earliest convenience of the emergency refills, and the prescription is not for a controlled substance. Provides that prescriptions may be refilled pursuant to the provisions for a period of time reasonably necessary for the pharmacist to secure prescriber authorization. Effective immediately. |
Licensed Activities and Pensions Comm. |
|
|
SB1815 |
Rose – Champaign, R |
Amends the Alcoholism and Other Drug Abuse and Dependency Act. Provides that any health care professional and any EMS Medical Director who, acting in good faith, directly or by standing order, prescribes or dispenses an opioid antidote to: (a) a patient who, in the judgment of the health care professional, is capable of administering the drug in an emergency, or (b) a person who is not at risk of opioid overdose but who, in the judgment of the health care professional, may be in a position to assist another individual during an opioid-related drug overdose and who has received basic instruction on how to administer an opioid antagonist shall not, as a result of his or her acts or omissions, except willful and wanton misconduct, be liable for civil damages when administering naloxone in an emergency situation. Amends the Good Samaritan Act. Provides that any law enforcement officer or fireman, any emergency medical technician, and any first responder who in good faith provides emergency care, including the administration of an opioid antagonist, without fee or compensation to any person shall not, as a result of his or her acts or omissions, except willful and wanton misconduct, be liable for civil damages when administering naloxone in an emergency situation. |
Human Services Comm. |
|
|
SB1844 |
Raoul – Chicago, D |
Amends the Illinois Insurance Code. Provides that all entities providing prescription drug coverage shall permit and apply a prorated daily cost-sharing rate to prescriptions that are dispensed by a pharmacy for less than a 30-day supply if the prescriber or pharmacist indicates the fill or refill could be in the best interest of the patient or is for the purpose of synchronizing the patient's chronic medications. Provides that no entity providing prescription drug coverage shall deny coverage for the dispensing of any drug prescribed for the treatment of a chronic illness that is made in accordance with a plan among the insured, the prescriber, and a pharmacist to synchronize the refilling of multiple prescriptions for the insured. Provides that no entity providing prescription drug coverage shall use payment structures incorporating prorated dispensing fees determined by calculation of the days' supply of medication dispensed. Provides that dispensing fees shall be determined exclusively on the total number of prescriptions dispensed. Establishes criteria for an entity conducting audits (either on-site or remotely) of pharmacy records. Provides that the Department of Insurance and Director of Insurance shall have the authority to enforce the provisions of the Act and impose financial penalties. Effective January 1, 2018. |
Insurance Comm. |
|
|
SB1888 |
McCann – Jacksonville, R |
Amends the Medical Assistance Article of the Illinois Public Aid Code. In addition to other specified actions required under the Code, requires a managed care community network that contracts with the Department of Healthcare and Family Services to establish, maintain, and provide a fair and reasonable reimbursement rate to pharmacy providers for pharmaceutical services, prescription drugs and drug products, and pharmacy or pharmacist-provided services. Provides that the reimbursement methodology shall not be less than the current reimbursement rate utilized by the Department for prescription and pharmacy or pharmacist-provided services and shall not be below the actual acquisition cost of the pharmacy provider. Requires a managed care community network to ensure that the pharmacy formulary used by the managed care community network and its contract providers is no more restrictive than the Department's pharmaceutical program. Effective July 1, 2018. |
Special Comm. on Oversight of Medicaid Managed Care |
|
|
SB1944 |
Nybo – Lombard, R |
Repeals the Hypodermic Syringes and Needles Act. Amends the Environmental Protection Act, the Drug Paraphernalia Control Act, and the Unified Code of Corrections to make conforming changes. Effective January 1, 2018. |
Public Health Comm. |
|
|
SB1971 Same as HB3572 |
Aquino – Chicago, D |
Amends the Illinois Insurance Code. Provides regulation for the creation of a list of drugs used to set the maximum allowable cost on which reimbursement to a pharmacy or pharmacist may be based. Provides that before a pharmacy benefits manager places or continues a particular drug on a maximum allowable cost list, the drug shall meet specified requirements. Provides for the duties of a pharmacy benefits manager in his or her use of a maximum allowable cost list. Provides for a reasonable administrative appeal procedure to allow pharmacies to challenge maximum allowable costs and reimbursements made under a maximum allowable cost for a specific drug. Provides that a pharmacy benefits manager shall not reimburse a pharmacy or pharmacist in this State in an amount less than the amount that the pharmacy benefits manager reimburses a pharmacy benefits manager affiliate for providing the same pharmacist services. Provides that a pharmacy or pharmacist may decline to provide pharmacist services to a patient or pharmacy benefits manager if, as a result of a maximum allowable cost list, a pharmacy or pharmacist is to be paid less than the pharmacy acquisition cost of the pharmacy providing pharmacist services. Provides that a violation of the provisions concerning maximum allowable cost lists and pharmacy benefits managers is a deceptive trade practice. Amends the Uniform Deceptive Trade Practices Act to make a conforming change. Defines terms. |
Insurance Comm. |
|
|
SB2011 |
Bivins – Dixon, R |
Amends the Illinois Controlled Substances Act. Provides that a registered pharmacist filling a prescription for an opioid substance listed in Schedule II may dispense the prescribed substance in a lesser quantity than the recommended full quantity indicated on the prescription if requested by the patient provided that the prescription complies with the requirements of the Act. Provides that the remaining quantity in excess of the quantity requested by the patient shall be void. Provides that if the dispensed quantity is less than the recommended full quantity, the pharmacist or his or her designee shall, within a reasonable time following a reduction in quantity but not more than 7 days, notify the prescribing practitioner of the quantity actually dispensed. Provides that nothing in this provision shall be interpreted to conflict with or supersede any other requirement established in the Act for a prescription of an opiate substance or any requirements or conditions for drug substitutions established in the Act. Effective immediately. |
Licensed Activities and Pensions Comm. |
|
|
SB2056 |
Rose – Champaign, R |
Amends the Pharmacy Practice Act. Provides that, beginning on January 1, 2022, all prescriptions orders for drugs or medical devices must be electronically transmitted to the patient's pharmacy of choice. Requires the Department of Financial and Professional Regulation to adopt rules governing the use of electronically transmitted prescription orders. |
Assignments Comm. |
|
|
|
|
|
|
|
|
HR0016 |
Gordon-Booth – Peoria, D |
Urges Congress to pass legislation in support of the establishment of VA emergency prescription refill programs nationwide to ensure that, in emergency situations, veterans may receive medication directly from their local pharmacy and VA facility. |
Veteran’s Affairs Comm. |
|
|
HR0030 |
Welch – Westchester, D |
Designates October 2017 as "Zombie Preparedness Month" in the State of Illinois, and urges all Illinoisans to educate themselves about natural disasters and take steps to create a stockpile of food, water, and other emergency supplies that can last up to 72 hours. |
Resolution Adopted. |
|
|
HR0059 |
Cassidy – Chicago, D |
Recognizes the importance of improving awareness of self-care and the value it represents to the citizens of Illinois. Supports increased consumer empowerment through the development of new nonprescription medicines and the appropriate switch of certain prescription medicines to nonprescription. Acknowledges that over-the-counter medicines can greatly improve and reduce costs to the public health system. Encourages consumers, healthcare practitioners, policymakers and regulators to communicate the benefits of self-care. Recognizes February of 2017 as Self-Care Month in Illinois. |
Human Services Comm. |
|
|
HR0088 |
Flowers – Chicago, D |
Urges the federal government to monitor the ever-increasing costs of prescription drugs and to take any necessary action to reduce the out-of-pocket expenses for those purchasing medications. |
Health Care Availability and Accessibility Comm. |
|
|
HR0116 |
McSweeney – Cary, R |
Declares opposition to raising the sales taxes on food and drugs. |
Revenue and Finance Comm. |
|
|
HB0239 SB0073 |
Flowers – Chicago, D |
Amends the Illinois Food, Drug and Cosmetic Act. Requires manufacturers of brand name or generic prescription drugs to notify State purchasers, health insurers, health care service plan providers, pharmacy benefit managers, and the General Assembly of specified increases in drug prices at least 60 days before such increase and the cost of specified new prescription drugs within 3 days after approval by the U.S. Food and Drug Administration. Provides that within 30 days after such notifications, prescription drug manufacturers shall report specified information to State purchasers, health insurers, health care service plan providers, pharmacy benefit managers, and the General Assembly. Provides that failure to report such information shall result in a specified civil penalty. Requires the General Assembly to conduct an annual public hearing on aggregate trends in prescription drug pricing. Provides that if the manufacturer of a prescription drug or its agent meets or otherwise communicates with a prescriber for the purpose of marketing a drug, then the manufacturer or its agent shall disclose to the prescriber if any ingredient in the drug it is marketing is known to pose a risk of dependency in humans. Makes other changes. |
Health Care Licenses Comm. |
|
|
HB240 |
Flowers – Chicago, D |
Amends the Third Party Prescription Programs Article of the Insurance Code, the Pharmacy Practice Act of 1987, and the Wholesale Drug Distribution Licensing Act. Prohibits the licensure, transference, use, or sale of any records relative to prescription information containing patient-identifiable or prescriber-identifiable data by any licensee or registrant of the Acts for commercial purposes. |
Health Care Licenses Comm. |
|
|
HB0274 |
Mussman – Schaumburg, D |
Amends the Pharmacy Practice Act. Provides that "practice of pharmacy" includes the prescribing and dispensing of hormonal contraceptive patches and self-administered oral hormonal contraceptives. Defines "hormonal contraceptive patch" as a transdermal patch applied to the skin of a patient, by the patient or by a practitioner, that releases a drug composed of a combination of hormones that is approved by the United States Food and Drug Administration to prevent pregnancy and "self-administered oral hormonal contraceptive" as a drug composed of a combination of hormones that is approved by the United States Food and Drug Administration to prevent pregnancy and that the patient to whom the drug is prescribed may take orally. Allows pharmacists to prescribe and dispense contraceptives to a person over 18 years of age and a person under 18 years of age only if the person has evidence of a previous prescription from a primary care or a women's health care practitioner. Requires the Department of Financial and Professional Regulation to adopt rules to establish standard procedures for pharmacists to prescribe contraceptives. Provides requirements for the rules to be adopted by the Department. Provides that all State and federal laws governing insurance coverage of contraceptive drugs and products shall apply to the provisions. |
Health Care Licenses Comm. |
Support |
|
HB0281 |
Flowers – Chicago, D |
Amends the Administration of Psychotropic Medications to Children Act. Provides that the Department of Children and Family Services shall adopt rules requiring the Department to distribute treatment guidelines on an annual basis to all persons licensed under the Medical Practice Act of 1987 to practice medicine in all of its branches. Provides that the Department shall prepare and submit an annual report to the General Assembly with specified information concerning the administration of psychotropic medication to persons for whom it is legally responsible. Amends the Medical Practice Act of 1987. Provides that the Department of Financial and Professional Regulation may revoke, suspend, place on probation, reprimand, refuse to issue or renew, or take any other disciplinary or non-disciplinary action as the Department may deem proper with regard to the license or permit of any person issued under the Act upon repeated acts of clearly excessive prescribing, furnishing, or administering psychotropic medications to a minor without a good faith prior examination of the patient and medical reason. |
Human Services Comm. |
|
|
HB0292 |
Olsen – Downers Grove, R |
Amends the Medical Assistance Article of the Illinois Public Aid Code. Provides that over-the-counter medications that are prescribed to a recipient of medical assistance by a physician, a physician assistant, a nurse practitioner, or any other medical care provider qualified to prescribe medications shall be covered under the State's medical assistance program. Provides that pharmacies providing prescribed over-the-counter medications shall be reimbursed at the same rate determined by the Department of Healthcare and Family Services for prescription medications covered under the State's medical assistance program. Requires the Department to establish guidelines and standards by administrative rule on the documentation, if any, a medical care provider must submit when prescribing an over-the-counter medication to a recipient of medical assistance. Effective immediately. |
Appropriations Human Services Comm. |
|
|
HB0312 |
Feigenholtz – Chicago, D |
Amends the Nurse Practice Act. In provisions concerning scope of practice, written collaborative agreements, temporary practice with a collaborative agreement, prescriptive authority with a collaborative agreement, titles, advertising, continuing education, and reports relating to professional conduct and capacity, changes references of "advanced practice nurse" and "APN" to "advanced practice registered nurse" and "APRN". Provides that a written collaborative agreement is required for all postgraduate advanced practice registered nurses until specific requirements have been met. Provides that postgraduate advanced practice registered nurses may enter into written collaborative agreements with collaborating advanced practice registered nurses or physicians (rather than collaborating physicians or podiatric physicians). In provisions concerning prescriptive authority for postgraduate advanced practice registered nurses, sets forth the requirements for postgraduate advanced practice registered nurses to have prescriptive authority and the limitations of such authority. Defines "full practice authority" and provides requirements for it to be granted to an advanced practice registered nurse. Removes provisions concerning advanced practice nursing in hospitals, hospital affiliates, or ambulatory surgical treatment centers, except the provision for anesthesia services and the provision requiring advanced practice registered nurses to provide services in accordance with other Acts. Makes other changes. Effective immediately. |
Health Care Licenses Comm. |
Opposed |
|
HB0313 |
Feigenholtz – Chicago, D |
Amends the Regulatory Sunset Act. Extends the repeal of the Nurse Practice Act from January 1, 2018 to January 1, 2028. Amends the Nurse Practice Act. Defines "focused assessment", "full practice authority", "oversight", and "postgraduate advanced practice nurse". Changes references of "advanced practice nurse" and "APN" to "advanced practice registered nurse" and "APRN" throughout the Act. Replaces provisions regarding nursing delegation with provisions that prohibit specified actions. Provides other guidelines for delegation of nursing activities and medication administration. Makes changes to education program requirements, qualifications for licensure, the scope of practice, and continuing education for LPN and RN licensees. Provides that a written collaborative agreement is required for all postgraduate advanced practice registered nurses until specific requirements have been met. Provides that postgraduate advanced practice registered nurses may enter into written collaborative agreements with collaborating advanced practice registered nurses or physicians (rather than collaborating physicians or podiatric physicians). In provisions concerning prescriptive authority for postgraduate advanced practice registered nurses, sets forth the requirements for postgraduate advanced practice registered nurses to have prescriptive authority and the limitations of such authority. Makes changes to provisions concerning the grounds for disciplinary action under the Act. Requires the Department of Public Health to prepare a report regarding the moneys appropriated from the Nursing Dedicated and Professional Fund to the Department of Public Health for nursing scholarships. Makes other changes. Effective immediately. |
Health Care Licenses Comm. |
Oppose |
|
HB0524 |
Wheeler – Crystal Lake, R |
Amends the Safe Pharmaceutical Disposal Act. Provides that pharmaceuticals disposed of under the Act may be destroyed in a drug destruction device. Amends the Environmental Protection Act. Expands the definition of "drug evidence" to include any used, expired, or unwanted pharmaceuticals collected under the Safe Pharmaceutical Disposal Act. Effective immediately. |
Police and First Responders Comm. |
|
|
HB0704 |
Bellock – Westmont, R |
Creates the Medicaid Smart Card Pilot Program Act. Requires the Director of the Department of Healthcare and Family Services to establish a Medicaid Smart Card Pilot Program to reduce the total amount of expenditures under the State's Medical Assistance Program. Provides that the pilot program shall be designed to reduce the average monthly cost under the State's Medical Assistance Program for recipients within the pilot program area by an amount that is at least sufficient to recover the cost of implementing the pilot program. Provides that the Director shall determine the geographic area to be included in the pilot program and may contract with an independent entity for the purpose of developing and implementing the pilot program. Contains provisions on required activities under the pilot program, including the distribution of Medicaid Smart Cards to designated recipients; measures the Department might take to implement the pilot program; annual evaluations; reporting requirements; extension or expansion of the pilot program; the confidentiality of health information; reports to the Inspector General; and rulemaking authority. |
Human Services Comm. Public Benefits Subc. |
|
|
HB0706 |
Bellock – Westmont, R |
Amends the Safe Pharmaceutical Disposal Act. Provides that in the absence of a police officer, State Police officer, coroner, or medical examiner at the scene of a death, a nurse or physician may dispose of unused medication found at the scene while engaging in the performance of his or her duties. Provides that anyone authorized to dispose of unused medications under the Act, and his or her employer, employees, or agents shall incur no civil liability, criminal liability, or professional discipline, except for willful or wanton misconduct, as a result of any injury arising from his or her good faith disposal or non-disposal of unused medication. Defines "nurse" and "physician". Amends the Medical Practice Act of 1987 and the Nurse Practice Act to make conforming changes. Effective immediately. |
Human Services Comm. Tort Liability Law Subcomm. |
|
|
HB0707 |
Bellock – Westmont, R |
Amends the Illinois Controlled Substances Act. Provides various penalties for knowingly withholding information from a practitioner from whom a person seeks to obtain a controlled substance or a prescription for a controlled substance. Provides that a health care practitioner with the intent to provide a controlled substance or combination of controlled substances that are not medically necessary to his or her patient or an amount of controlled substances that is not medically necessary for his or her patient, may not provide a controlled substance or a prescription for a controlled substance by misrepresentation, fraud, forgery, deception, subterfuge, or concealment of a material fact. Provides that a violation is a Class 4 felony for the first offense and a Class 3 felony for each subsequent offense. The fine for the first offense shall be not more than $100,000. The fine for each subsequent offense shall not be more than $200,000. |
Judiciary – Criminal Comm. Sentencing, Penalties and Criminal Procedure Sub. Comm. |
Support |
|
HB1796 |
Harris – Chicago, D |
Creates the Health Insurance Claims Assessment Act. Imposes an assessment of 1% on claims paid by a health insurance carrier or third-party administrator. Provides that the moneys received and collected under the Act shall be deposited into the Healthcare Provider Relief Fund and used solely for the purpose of funding Medicaid services provided under the medical assistance programs administered by the Department of Healthcare and Family Services. |
Appropriations – Human Services Comm. |
|
|
HB2392 |
Flowers – Chicago, D |
Amends the Pharmacy Practice Act. Requires that at least one registered pharmacy technician be on duty whenever the practice of pharmacy is conducted. Requires that pharmacies fill no more than 10 prescriptions per hour. Requires 10 pharmacy technician hours per 100 prescriptions filled. Prohibits pharmacies from requiring pharmacists to participate in advertising or soliciting activities that may jeopardize patient health, safety, or welfare and any activities or external factors that interfere with the pharmacist's ability to provide appropriate professional services. Provides that a pharmacist shall receive specified break periods. Provides that a pharmacy may not require a pharmacist to work during a break period, shall make available a break room meeting specified requirements, shall keep a complete and accurate record of the break periods and may not require a pharmacist to work more than 8 hours a workday. Provides for enforcement and penalties. Provides whistleblower protections for an employee of a pharmacy if the pharmacy retaliates against the employee for certain actions. Requires pharmacies to maintain a record of any errors in the receiving, filling, or dispensing of prescriptions. |
Health Care Licenses Comm. |
Oppose |
|
HB2436 |
Flowers – Chicago, D |
Creates the Illinois Medicare for All Health Care Act. Provides that all individuals residing in the State are covered under the Illinois Health Services Program for health insurance. Sets forth the health coverage benefits that participants are entitled to under the Program. Sets forth the qualification requirements for participating health providers. Sets forth standards for provider reimbursement. Provides that it is unlawful for private health insurers to sell health insurance coverage that duplicates the coverage of the Program. Provides that investor-ownership of health delivery facilities is unlawful. Provides that the State shall establish the Illinois Health Services Trust to provide financing for the Program. Sets forth the requirements for claims billing under the Program. Provides that the Program shall include funding for long-term care services and mental health services. Provides that the Program shall establish a single prescription drug formulary and list of approved durable medical goods and supplies. Creates the Pharmaceutical and Durable Medical Goods Committee to negotiate the prices of pharmaceuticals and durable medical goods with suppliers or manufacturers on an open bid competitive basis. Sets forth provisions concerning patients' rights. Provides that the employees of the Program shall be compensated in accordance with the current pay scale for State employees and as deemed professionally appropriate by the General Assembly. Effective January 1, 2018. |
Health Care Availability and Accessibility Comm. |
|
|
HB2511 |
Feigenholtz – Chicago, D |
Amends the Medical Assistance Article of the Illinois Public Aid Code. Provides that drugs prescribed for residents of licensed long-term care facilities shall not be subject to prior approval as a result of the 4-prescription limit. |
Appropriations – Human Services Comm. |
|
|
HB2531 |
Hammond – Macomb, R |
Amends the Illinois Food, Drug and Cosmetic Act. Deletes provisions requiring manufacturers to provide the Director of Public Health with a notification containing product technical bioequivalence information no later than 60 days prior to specified generic drug product substitution. Effective immediately. |
Human Services Comm. |
|
|
HB2708 |
Demmer – Rochelle, R |
Amends the Illinois Controlled Substances Act. Provides that the Department of Human Services may release information received by the central repository to select representatives of the Department of Children and Family Services through the indirect online request process. Provides that access shall be established by the Prescription Monitoring Program Advisory Committee by rule. |
Human Services Comm |
|
|
HB2742 |
Zalewski – Riverside, D |
Amends the Pharmacy Practice Act. Requires the Department of Financial and Professional Regulation to adopt rules requiring pharmacy prescription systems, including, but not limited to, electronic systems, to contain mechanisms to require prescription discontinuation orders to be forwarded to a pharmacy, to require patient verification features for pharmacy automated prescription refills, and to require that automated prescription refills notices clearly communicate to patients the medication name, dosage strength, and any other information required by the Department governing the use of automated dispensing and storage systems. Provides that the rules shall ensure that discontinued medications are not automatically dispensed to a patient by a pharmacist or by any automatic refill dispensing system whether prescribed through electronic or paper prescriptions. Effective immediately. |
Health Care Licenses Comm. |
|
|
HB2908 same as SB1596 |
Bellock – Westmont, R |
Amends the Medical Assistance Article of the Illinois Public Aid Code. In provisions concerning medical assistance for the treatment of alcohol dependence or opioid dependence, provides that on or after July 1, 2017 such coverage may be subject to utilization controls or prior authorization mandates consistent with the most current edition of the American Society of Addiction Medicine's National Practice Guideline for the Use of Medications in the Treatment of Addiction Involving Opioid Use, as now or hereafter revised, or any successor publication (rather than on or after July 1, 2015 such coverage shall not be subject to any (1) utilization control, other than those established under the American Society of Addiction Medicine patient placement criteria, (2) prior authorization mandate, or (3) lifetime restriction limit mandate). Provides that on or after July 1, 2017, opioid antagonists prescribed for the treatment of an opioid overdose may be subject to (A) utilization controls or (B) prior authorization mandates consistent with the most current edition of the American Society of Addiction Medicine's National Practice Guideline for the Use of Medications in the Treatment of Addiction Involving Opioid Use, as now or hereafter revised, or any successor publication. |
Human Services Comm. |
|
|
HB2951 |
Williams – Chicago, D |
Amends the Medical Practice Act of 1987. Except when dispensing manufacturers' samples or other legend drugs in a maximum 72 hour supply, requires persons licensed under the Act to label samples consistent with specified labeling requirements (rather than maintain a book or file of prescriptions as required in the Pharmacy Practice Act). Effective immediately. |
Health Care Licenses Comm. |
|
|
HB2956 same as SB1609 |
McAsey – Romeoville, D |
Amends the Illinois Insurance Code, the State Employees Group Insurance Act of 1971, the Counties Code, the Illinois Municipal Code, the School Code, the Health Maintenance Organization Act, the Limited Health Service Organization Act, the Voluntary Health Services Plans Act, and the Illinois Public Aid Code. Prohibits insurers from requiring that a covered individual first use an opioid analgesic drug product without abuse-deterrence labeling claims before providing coverage for an abuse-deterrent opioid analgesic drug product. |
Insurance: Health and Life Comm. |
|
|
HB2957 same as SB1546 |
Fine – Glenview, D |
Amends the Illinois Insurance Code. Provides that every policy of accident and health insurance amended, delivered, issued, or renewed after the effective date of the amendatory Act that provides coverage for prescription drugs shall provide for synchronization of prescription drug refills on at least one occasion per insured per year provided that certain conditions are met. Requires insurers to provide prorated daily cost-sharing rates when necessary. Makes conforming changes in the State Employees Group Insurance Act of 1971, the Counties Code, the Illinois Municipal Code, the School Code, the Health Maintenance Organization Act, the Limited Health Services Organization Act, the Voluntary Health Services Plan Act, and the Illinois Public Aid Code. Effective immediately. |
Insurance: Health and Life Comm. |
|
|
HB3285 |
Rita – Blue Island, D |
Amends the Illinois Insurance Code. Provides that all entities providing prescription drug coverage shall permit and apply a prorated daily cost-sharing rate to prescriptions that are dispensed by a pharmacy for less than a 30-day supply if the prescriber or pharmacist indicates the fill or refill could be in the best interest of the patient or is for the purpose of synchronizing the patient's chronic medications. Provides that no entity providing prescription drug coverage shall deny coverage for the dispensing of any drug prescribed for the treatment of a chronic illness that is made in accordance with a plan among the insured, the prescriber, and a pharmacist to synchronize the refilling of multiple prescriptions for the insured. Provides that no entity providing prescription drug coverage shall use payment structures incorporating prorated dispensing fees determined by calculation of the days' supply of medication dispensed. Provides that dispensing fees shall be determined exclusively on the total number of prescriptions dispensed. Establishes criteria for an entity conducting audits (either on-site or remotely) of pharmacy records. Provides that the Department of Insurance and Director of Insurance shall have the authority to enforce the provisions of the Act and impose financial penalties. Effective January 1, 2018. |
Insurance: Health and Life Comm. |
|
|
HB3388 |
Gordon-Booth – Peoria, D |
Amends the Home Medical Equipment and Services Provider License Act and the Pharmacy Practice Act. Requires a home medical equipment and services provider that provides or a pharmacist that dispenses pressurized oxygen or any oxygen delivery system to a patient to inform the municipal fire department or fire protection district that serves the patient of the patient's oxygen use in his or her home in case of a fire. |
Fire and Emergency Services Comm. |
|
|
HB3462 same as SB0902 |
Zalewski – Riverside, D |
Amends the Regulatory Sunset Act. Extends the repeal date of the Pharmacy Practice Act from January 1, 2018 to January 1, 2028. Amends the Pharmacy Practice Act. Provides that all applicants and licensees shall provide a valid address and email address, which shall serve as the address and email address of record, and shall inform the Department of Financial and Professional Regulation of any change of address or email address through specified means. Provides for the licensure (rather than registration) of registered pharmacy technicians, registered certified pharmacy technicians, and pharmacists, and makes conforming changes. Removes provision allowing each member of the State Board of Pharmacy to receive a per diem payment in an amount determined from time to time by the Secretary of Financial and Professional Regulation for attendance at meetings of the Board and conducting other official business of the Board. Changes references to "Director" to references to "Secretary" or "Department" throughout the Act. Eliminates the position of deputy pharmacy coordinator. Makes changes in provisions concerning definitions, duties of the Department, inactive status, pharmacists in charge, nonresident pharmacy licenses, record retention, automated pharmacy systems, remote prescription processing, and discipline. Makes other changes. Effective immediately. |
Health Care Licenses Comm. |
|
|
HB3472 |
Soto – Chicago, D |
Amends the Regulatory Sunset Act. Extends the repeal date of the Nurse Practice Act from January 1, 2018 to January 1, 2028. Amends the Nurse Practice Act. Eliminates the position of Assistant Nursing Coordinator. Eliminates the Advanced Practice Nursing Board. Provides that the Department of Financial and Professional Regulation may provide notice to a licensee or applicant by certified or registered mail to the address of record or by email to the email address of record. Provides provisions for change of address of record and email address of record, application for license, confidentiality of any information collected by the Department in the course of an examination or investigation of a license or applicant, and disposition by a consent order. Changes references to "advanced practice nurse" to references to "advanced practice registered nurse" throughout the Act and other Acts. Changes references to "Illinois Center for Nursing" to references to "Illinois Nursing Workforce Center". Makes changes concerning definitions, application of the Act, unlicensed practice, prohibited acts, Department powers and duties, nursing delegation, qualifications for LPN, RN, and APRN licensure, RN education program requirements, grounds for disciplinary action, intoxication and drug abuse, the Nursing Dedicated and Professional Fund, investigations, notices, hearings, use of stenographers and transcripts, review under the Administrative Review Law, certification of records, the Center for Nursing Advisory Board, and medication aide licensure requirements. Removes provisions concerning registered nurse externship permits, rosters, liability of the State, hearing officers, and orders for rehearings. Makes other changes. Effective immediately. |
Health Care Licenses Comm. |
|
|
HB3479 |
Feigenholtz – Chicago, D |
Amends the Medical Assistance Article of the Illinois Public Aid Code. In addition to other specified actions required under the Code, requires a managed care community network that contracts with the Department of Healthcare and Family Services to establish, maintain, and provide a fair and reasonable reimbursement rate to pharmacy providers for pharmaceutical services, prescription drugs and drug products, and pharmacy or pharmacist-provided services. Provides that the reimbursement methodology shall not be less than the current reimbursement rate utilized by the Department for prescription and pharmacy or pharmacist-provided services and shall not be below the actual acquisition cost of the pharmacy provider. Requires a managed care community network to ensure that the pharmacy formulary used by the managed care community network and its contract providers is no more restrictive than the Department's pharmaceutical program. Effective July 1, 2018. |
Human Services Comm. |
|
|
HB3572 same as SB1971 |
Soto – Chicago, D |
Amends the Illinois Insurance Code. Provides regulation for the creation of a list of drugs used to set the maximum allowable cost on which reimbursement to a pharmacy or pharmacist may be based. Provides that before a pharmacy benefits manager places or continues a particular drug on a maximum allowable cost list, the drug shall meet specified requirements. Provides for the duties of a pharmacy benefits manager in his or her use of a maximum allowable cost list. Provides for a reasonable administrative appeal procedure to allow pharmacies to challenge maximum allowable costs and reimbursements made under a maximum allowable cost for a specific drug. Provides that a pharmacy benefits manager shall not reimburse a pharmacy or pharmacist in this State in an amount less than the amount that the pharmacy benefits manager reimburses a pharmacy benefits manager affiliate for providing the same pharmacist services. Provides that a pharmacy or pharmacist may decline to provide pharmacist services to a patient or pharmacy benefits manager if, as a result of a maximum allowable cost list, a pharmacy or pharmacist is to be paid less than the pharmacy acquisition cost of the pharmacy providing pharmacist services. Provides that a violation of the provisions concerning maximum allowable cost lists and pharmacy benefits managers is a deceptive trade practice. Amends the Uniform Deceptive Trade Practices Act to make a conforming change. Defines terms. |
Health Care Licenses Comm. |
|
|
HB3607 |
Evans – Chicago, D |
Amends the Illinois Insurance Code. Provides procedures for conducting pharmacy audits under the Third Party Prescription Programs Article. Prohibits an audit entity from using extrapolation to calculate penalties or amounts to be charged back, unless otherwise required by federal requirements. Defines terms. Contains provisions concerning notice of an audit, confidentiality, records, audit reporting, compensation, interest accrual, and appeal of a final audit report. Makes other changes. Provides that all entities providing prescription drug coverage shall permit and apply a prorated daily cost-sharing rate to prescriptions that are dispensed by a pharmacy for less than a 30-day supply if the prescriber or pharmacist indicates the fill or refill could be in the best interest of the patient or is for the purpose of synchronizing the patient's chronic medications. Provides that no entity providing prescription drug coverage shall deny coverage for the dispensing of any drug prescribed for the treatment of a chronic illness that is made in accordance with a plan among the insured, the prescriber, and a pharmacist to synchronize the refilling of multiple prescriptions for the insured. Provides that no entity providing prescription drug coverage shall use payment structures incorporating prorated dispensing fees determined by calculation of the days' supply of medication dispensed. Provides that dispensing fees shall be determined exclusively on the total number of prescriptions dispensed. Provides that the Department of Insurance and the Director shall have the authority to enforce the provisions of the Act and impose financial penalties. Effective immediately. |
Health Care Licenses Comm. |
|
|
HB3833 |
Brady – Normal, R |
Amends the Care of Students with Diabetes Act, the Illinois Insurance Code, the Health Maintenance Organization Act, the Limited Health Service Organization Act, the Managed Care Reform and Patient Rights Act, the Voluntary Health Services Plans Act, and the Health Care Services Lien Act to add pharmacy or pharmacist-provided services to the types of health services under the Acts and to add pharmacists as health care providers or health care professionals under the Acts. Effective January 1, 2018. |
Executive Comm. |
|
Educational Affairs
Implementation and Evaluation of a Student Mentorship Program at a College of Pharmacy
by Shaziya Barkat, Pharm D Candidate, Midwestern University Chicago College of Pharmacy, SSHP President; Jen Phillips, PharmD, BCPS, FCCP Associate Professor, Midwestern University Chicago College of Pharmacy, SSHP Co-Advisor; Kathy Komperda, PharmD, BCPS Associate Professor, Midwestern University Chicago College of Pharmacy, SSHP Advisor
Introduction
As humans, we’re always growing and learning. Even the most experienced professional needs guidance, and an often overlooked yet beneficial resource to help oneself develop is mentorship. Mentorship involves a relationship between at least two individuals – a more experienced person (“mentor”) and a less experienced person (“mentee”) that is typically long-term and often occurs in a professional setting.1 Mentoring has largely been correlated with positive outcomes for both the mentor and the mentee.2 For example, in one study analyzing the impact of a pharmacist mentorship program, pharmacist mentees reported an increased level of self-perceived competency and confidence and both the mentors and the mentees reported an increase in job satisfaction as a result of the program.2 This impact is not necessarily limited to pharmacists or adults. A multi-disciplinary meta-analysis found that mentoring was associated with a wide range of positive outcomes including behavioral, attitudinal, health-related, motivational, and career outcomes.3
Implementation of a Pharmacy Student Mentorship Program
In September 2015, the Midwestern University Chicago College of Pharmacy (MWU-CCP) Illinois Council of Health-System Pharmacists (ICHP) student chapter launched a new college-wide mentorship program on the Downers Grove Campus. The mission of this program was to ease the transition of incoming student pharmacists and to foster professional relationships among all levels of students in the College of Pharmacy.
To find the
best fit, first-year student pharmacists were matched with either a second- or
third-year student pharmacist based on a questionnaire assessing specific
preferences. The questionnaire focused on interests, professional goals,
self-identified strengths and weaknesses, and availability. Inclusion criteria
and requirements of the program are outlined in Table 1. A total of 98
students, 49 mentors and 49 mentees, participated in this program in the
2015-2016 academic year. Approximately 136 hours of mentorship were logged during that time.
Table 1:
Inclusion Criteria and Mentorship Program Requirements
Inclusion
Requirements
• Enrolled in pharmacy program at MWU
• MWU ICHP member
• PS-1s as mentees
• PS-2s or PS3s as mentors
• Program orientation attendance
• At least one 30 minute meeting between mentor-mentee meeting per academic quarter
• Attendance at the end of the year mentorship social
*PS-1s, 2s, and 3s=Pharmacy Student-year 1, 2 and 3 respectively
Evaluation of a Pharmacy Student Mentorship Program
Evaluating a
mentorship program for areas of development can help both interested mentors
and mentees gain even more from their experience. In an effort to do this, the
MWU-CCP ICHP Mentorship Committee conducted a year-long quality improvement
study, which was classified as exempt by the Midwestern University Institutional
Review Board. The objective of this initiative was to identify benefits and
challenges that participants experienced while participating in the program and
to determine areas for improvement.
As part of the evaluation, all participants were provided an end-of-year survey. Out of 98 participants, 69 participants (70%) including 33 mentors and 36 mentees participated in the anonymous survey. The survey included questions for mentors and mentees as well as some questions that both groups answered. The questions targeted the subjects’ satisfaction and professional development as well as the program’s quality and efficacy in the mentor/mentee match process.
Benefits of the Program
Table 2 shows the results for the questions that both mentors and mentees answered. Overall, 100% of mentor and mentee respondents indicated that they were satisfied with the student mentorship program and 100% of mentors and 94% of mentee respondents indicated that they would recommend the program to others. More than 90% of participants who responded indicated that they were satisfied with the matching process, and the vast majority in both groups noted that the program increased confidence when networking. Most survey respondents indicated that they were interested in having more organized social events within the mentorship program.
Table 2: Results of Student Mentorship Program Quality Improvement Survey
|
|
Mentors (N=33) |
Mentees (N=36) |
||
|
A/SA N (%) |
D/SD N (%) |
A/SA N (%) |
D/SD N (%) |
|
|
Satisfied with program |
35 (100) |
0 (0) |
36 (100) |
0 (0) |
|
Would recommend program |
33 (100) |
0 (0) |
34 (94) |
1 (3) |
|
Satisfied with matching process |
30 (91) |
3 (9) |
33 (92) |
3 (8) |
|
Interested in social events |
29 (88) |
4 (12) |
32 (89) |
2 (5) |
|
Program increased confidence when networking |
29 (88) |
3 (19) |
35 (100) |
0 (0) |
A=Agree, SA = Strongly Agree, D=Disagree, SD=Strongly Disagree
Regarding the questions geared specifically toward mentors, 29 (91%) of respondents agreed that the program prepared them to be a mentor and 31 (97%) agreed that the program helped them build leadership skills. Regarding the questions geared specifically toward mentees, 33 (92%) of respondents agreed that the program prepared them to be a mentee and 30 (88.2%) agreed that participation in the program helped them learn more about future career opportunities. In addition, 31 (89%) of respondents believed that participation in the program also helped them academically.
Challenges
of the Program
In addition to structured questions, participants were also provided an opportunity to provide free response comments about the program. A summary of comments provided is included in Table 3. Some of the free response comments were consistent with the structured question responses summarized in Table 2. However, there were some opportunities for improvement that were noted in these comments. Throughout the program, mentor-mentee pairs were given the autonomy to gather socially on their own. However, our evaluation demonstrated that participants preferred planned social events throughout the program. It was also determined that there should be clear communication regarding overall expectations from both the mentor and mentee perspectives. In order to address these comments, moving forward the program will provide more mentorship socials and include more detailed training for mentors and mentees prior to the start of mentorship years through additional workshops.
Table 3: Free Response Comments about Mentorship
Program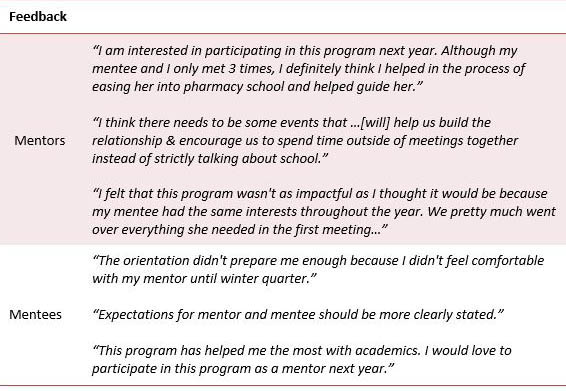
Conclusions
Mentorship can be beneficial for both the mentor and mentee. It can help individuals set and achieve professional goals, overcome personal challenges, learn new skills, or simply obtain new perspectives. Establishing a successful student mentorship program involves using continuous assessment to identify areas for improvement and ensure that an optimal mentor-mentee relationship is achieved. MWU-CCP plans on continuing this successful student mentorship program and we look forward to continuing to improve the quality of the program.
References
1. Sambunjak D, Marusic A. Mentoring. What’s in a name? JAMA. 2009(302):2591-2.
2. Nieuwstraten C, Huh A, Liu G, et al. Developing, implementing, and evaluating a formal pharmacist mentorship program. Can J Hosp Pharm. 2011;64(2):124-30.
3. Eby LT, Allen TD, Evans SC, et al. Does mentoring matter? A multidisciplinary meta-analysis comparing mentored and non-mentored individuals. J Vocat Behav. 2008;72(2):254-267.
Educational Affairs Poster Abstracts
2017 ICHP-MSHP Spring Meeting Poster Abstracts
EDITOR’S NOTE: For a detailed list of all posters as presented at the 2017 ICHP-MSHP Spring Meeting, please refer to the Spring Meeting Handouts Page, http://www.ichpnet.org/events/spring_meeting/2017/program_handouts.php.
All research was to have results and conclusions by the time of presentation. This may not be reflected in the posted abstracts below.
PLATFORM PRESENTATIONS
1. Breaking Real and Perceived Barriers to Voluntary Reporting of Safety Events by Pharmacy Personnel in an Acute Care Institution
2. Student Attitudes and Behaviors on Utilization of a Virtual Dispensing Software in a Healthcare Communications Course
ORIGINAL
1. Utilizing Existing Staff to Address Antimicrobial Stewardship Needs in a Small Urban Community Hospital (Poster #9)
2. The Optimization of Automated Dispensing Cabinets in an Academic Medical Center (Poster #10)
3. Medication Utilization and Patient Falls Correlated with the Use of Melatonin and Zolpidem in the Hospital (Poster #11)
4. Most Valuable Components of Residency Training at the University of Chicago Medicine (Poster #28 – not presented)
5. Management of Heparin Infusions in the Obese Population (Poster #30)
ENCORE
1. Evaluation of Sustained Virologic Response Rates after Hepatitis C Virus Treatment among a Diverse Patient Population at an Urban Academic Medical Center (Poster #13 – not presented)
2. Pharmacy Desensitization in a Collaborative Practice with Allergy Clinic (Poster #34)
STUDENT
1. The Deprescribing Conversation Project: Giving Nurses the “Words” (Poster #18)
2. Reducing Polypharmacy: Deprescribing at an Academic Medical Center (Poster #36)
3. Fall Risk Assessments in a Community-based Senior Outreach Program (Poster #39)
4. Dose Adjustments of Thiopurines in Patients Based on Thiopurine Methyltransferase Activity (Poster #41)
5. The Impact of Pharmacist-Driven Pantoprazole to Famotidine Substitution Protocol on Rates of Hospital-Acquired Clostridium difficile (Poster #42 – not presented)
6. Evaluation of Pain Medication Management in Patients Admitted to a Large Academic Hospital (Poster #43 – not presented)
*****************************************************************************************
ICHP Poster Presentations - Platform Presentation 1
Category: Encore
Title: Breaking Real and Perceived Barriers to Voluntary Reporting of Safety Events by Pharmacy Personnel in an Acute Care Institution
Purpose: Purpose Voluntary incident reporting by healthcare personnel discloses adverse events and errors so patient safety and quality of care can be tracked and improved. However, it is estimated that adverse events in healthcare systems are underreported at an annual rate of 50 to 96%. Barriers to reporting include fear of individual or organizational repercussion; a belief that reporting errors can measure practitioner competence; and potential legal concerns associated with error reporting. The purpose of this study is to assess perceived and real barriers to voluntary reporting of safety events by pharmacy personnel at Northwestern Memorial Hospital (NMH) in Chicago, IL.
Methods: An anonymous survey on attitudes and barriers to reporting in the Northwestern Events Tracking System (NETS) was created in SurveyMonkey and emailed in September 2016 to 171 pharmacists and 112 technicians at NMH via email listservs. The survey consisted of 17 questions on demographics, awareness of event reporting, and concerns with event reporting using a Likert scale. The same survey will be emailed out to the same group after education and process improvement(s) have been implemented, in order to measure changes in awareness of the NETS process and any changes in barriers to use. Prior to administration of the survey, the number of medication safety events (those that are categorized as “Adverse Drug Reactions” and “Medication/Fluid”) reported in NETS by pharmacists and pharmacy technicians were measured from all reports submitted under these categories from December 2015 through February 2016. These data will be collected again after education and process improvement(s) are implemented, in order to assess any changes in reporting by pharmacy personnel.
Results: Prior to this survey, 34 medication safety event reports were made by pharmacists and 3 were made by pharmacy technicians in the measured 3 month period. Of the 283 pharmacy personnel who received the survey, 114 completed it (40% response rate). A majority of respondents are pharmacists (72%), and a majority work in an inpatient setting (83%). Nearly all respondents are aware of the NETS (98%) and of how to access and submit reports (96%), but many claim they rarely (34%) or never (18%) report an event through the NETS. The top 4 identified barriers to reporting based on those who responded “Strongly Agree” or “Agree” to statements about perceived barriers are as follows: fear of distrust among colleagues for submitting a report involving them (36%); a lack of follow-up after an incident report is submitted (34%); concern that information can be traced back to the person who submitted the report (32%); and a concern that disciplinary action will be taken upon the person involved in the event based on the report (28%).
Conclusions: Survey results demonstrate that fear of repercussion, lack of anonymity, and distrust among colleagues are major barriers to event reporting. Fostering a just culture through emphasis on patient safety both at the level of pharmacy leadership and throughout the department, along with streamlining management of events and providing follow-up on improvements made should help to break these barriers.
Submitting Author: Lara Ellinger, PharmD, BCPS
Organization: Northwestern Memorial Hospital
Authors: Lara Ellinger, PharmD, BCPS, Drug Information and Medication Safety Pharmacist; Tina Lertharakul, PharmD Candidate, Midwestern University; Katherine Gauen, PharmD, Pharmacy Administration PGY2 Resident, Northwestern Memorial Hospital.
***************************************************************************************
ICHP Poster Presentations - Platform Presentation 2
Winner: Best Platform Presentation 2017
Category: Student Research Complete
Title: Student Attitudes and Behaviors on Utilization of a Virtual Dispensing Software in a Healthcare Communications Course
Purpose: Student Attitudes and Behaviors on Utilization of a Virtual Dispensing Software in a Healthcare Communications Course Purpose: The Accreditation Council for Pharmacy Education (ACPE) requires that medication preparation and dispensing be incorporated into didactic coursework. While it is taught and practiced in the earlier years of pharmacy education, it is not until students are on Advanced Pharmacy Practice Experiences (APPEs) that the skills and knowledge are tested in a real world environment. The actions of verifying and dispensing medications only comprise a small portion of the activities required during the APPE community rotation. To better prepare students for the potential role of dispensing in their future practice, aspects of dispensing should be incorporated early on in the curriculum. Previous studies using a limited population of pharmacy students have shown students are willing to use a virtual dispensing software and perceive it to be helpful. The objective of our study is to explore student perceptions and use of virtual dispensing software in a broader, larger student population.
Methods: A virtual dispensing software (MyDispense) was incorporated into a required communications course. MyDispense was developed by Monash University in Australia for use in their pharmacy curriculum and has been modified for use in other countries, including the US. The exercises used in this course focused on common problems seen in community practice, including contacting the prescriber for clarification, drug interactions between different prescription medications, and drug interactions between prescription and over the counter medications. This questionnaire-based study was conducted at Midwestern University Chicago College of Pharmacy in Downers Grove, Illinois. All third year pharmacy students who had used MyDispense as part of the communications course were eligible to participate. The questionnaire collected information regarding student usage of MyDispense, perceptions of the software, and demographics. The questionnaire was administered via SurveyMonkey at the beginning of a required course session once all MyDispense assignments and quizzes were completed for the course. Descriptive statistics were utilized for results of this study. This project was approved by the Midwestern University IRB.
Results: One hundred sixty-two students participated in the study, resulting in a 91.5% response rate. The majority was female (75%) and had a bachelor’s degree (66%). The median age was twenty-five years old. Most students had pharmacy work experience (85%), with a majority of that experience being in community pharmacy (83%). One hundred and four students (64%) completed at least 80% of the practice exercises. One hundred and thirty-six students (85%) felt that using MyDispense was a positive learning experience and one hundred and thirty-nine students (87%) stated that MyDispense made them more aware of the dispensing process, including performing tasks such as checking for drug interactions, contacting the prescriber as necessary, and asking the patient relevant questions. Additionally, one hundred and forty-eight students (92.5%) felt that there would be a benefit from using MyDispense earlier on in the curriculum.
Conclusions: The implementation of a virtual dispensing program in a required course was received positively, as shown by the usage of the students. A majority of students found a significant benefit from using MyDispense. Despite that most of these students had previous and current community pharmacy work experience, most students achieved a better insight into the dispensing process and into the role of the pharmacist in the community setting.
Submitting Author: Michael Serlin, PharmD Candidate
Organization: Midwestern University Chicago College of Pharmacy
Authors: Michael William Serlin- PharmD Candidate, Midwestern University Chicago College of Pharmacy; Jennifer Mazan, PharmD, Professor, Midwestern University Chicago College of Pharmacy; Kathy E. Komperda, PharmD, BCPS, Professor, Midwestern University Chicago College of Pharmacy.
************************************************************************************
ICHP Poster Presentations – Original 1
(presented as Poster #9)
Category: Original-Research in Progress
Title: Utilizing Existing Staff to Address
Antimicrobial Stewardship Needs in a Small Urban Community Hospital
Purpose: Antimicrobial stewardship is a necessary responsibility in healthcare facilities to control the emergence of bacterial resistance, health care costs, and healthcare-acquired infection rates. The Joint Commission adopted a new Medication Management standard (MM.09.01.01) to define required elements of Antimicrobial Stewardship Programs (ASPs), effective 1/1/17. In preparation, the study site’s Pharmacy Department sought to develop an ASP pilot with existing pharmacy staff. The purpose was to determine if an internal change made to the staffing model, allowing a lead pharmacist dedicated time to perform ASP activities, was effective in reducing the duration of broad-spectrum antibiotics and overall anti-infective use.
Methods: The pilot was conducted at a small community hospital with an average daily census of 69 patients comprised of 40% behavioral health patients from 6/13/16 to 12/13/16 compared to a pre-intervention period of 1/1/15 to 12/31/15. Before pilot initiation, the feasibility of dedicating an entire shift to ASP efforts was determined by evaluating the average number of orders processed on weekdays versus weekends. A weekend shift was moved to Monday to assign an existing staff member as the designated lead ASP pharmacist for the department. ASP presentations, readings, and competency questions provided further training for pharmacy staff. The lead ASP pharmacist reviewed antimicrobial drug therapy based on daily trigger reports and monitored for clinical response. Interventions focused on drug-bug mismatch, de-escalation, discontinuation, and duration of therapy opportunities. The pharmacy staff was encouraged to make antimicrobial stewardship interventions throughout the week. The number of pharmacist-driven ASP interventions and duration of therapy for the most impacted broad-spectrum antibiotics were the primary outcomes. Cost per adjusted patient days for anti-infectives was the secondary outcome.
Results: Research in Progress. There was a 6-fold increase in the number of antimicrobial stewardship interventions with 310 interventions in the 6-month post-intervention period as compared to 51 interventions in the 12-month pre-intervention period. The two most impacted antibiotics by this pilot were levofloxacin (90 interventions) and piperacillin-tazobactam (38 interventions). The average durations of therapy decreased by 4% and 1% for levofloxacin and piperacillin-tazobactam respectively in the post-intervention versus the pre-intervention periods. Average anti-infective cost per adjusted patient day decreased from $4.94 to $3.10 in the pre-intervention versus the post-intervention period. (Additional data to be presented at the meeting.)
Conclusions: Research in Progress. In hospital settings across the United States, ASPs are being created to optimize the use of antibiotics, prevent resistance and minimize adverse events. As shown in the pilot, for smaller community hospitals, creating internal infrastructure to support ASP efforts can still make an impact. (Additional data to be presented at the meeting.)
Submitting Author: Zeina Samara, PharmD
Organization: Westlake Hospital
Authors: Zeina E. Samara, PharmD, Clinical Pharmacist Tenet Healthcare - Westlake Hospital; Dan V. Ciarrachi, RPh, Clinical Pharmacist Tenet Healthcare - Westlake Hospital; Charlene Hope Henry, PharmD, MS, BCPS, Quality and Safety Pharmacy Manager, Chicago Market, Tenet Healthcare - MacNeal, Weiss, West Suburban, Westlake; Stacy Thomas Scaria, PharmD, Clinical Pharmacist Tenet Healthcare – West Lake Hospital; Deanna McMahon Horner, PharmD, BCPS, Clinical Pharmacy Manager, UnitedHealthcare Medicare & Retirement, Part D STARs.
**************************************************************************************
ICHP Poster Presentations – Original 2
(presented as Poster #10)
Category: Original-Research in Progress
Title: The Optimization of Automated
Dispensing Cabinets in an Academic Medical Center
Purpose: The University of Chicago’s pharmacy department strives to direct operations around the effective use of automation and technology. This project was primarily conducted to ensure the proper utilization of current automation and technology, specifically automated dispensing cabinets (ADCs), in the most efficient manner to meet the patient care needs of the medical center. The University of Chicago Medical Center has contemporary pharmacy automation solutions in place, some of which include ADCs. An attempt to maximize the efficiency of the drug distribution technology was made, focusing in on the medication dispensing carousels located within the pharmacy and the automated dispensing cabinets located in the adult patient care areas throughout the medical center (The Center for Care and Discovery and the Mitchell Hospital). The primary objective of the optimization efforts were to maximize the amount of medications dispensed as common stock instead of patient specific doses from the ADCs, which ultimately reduces the time and effort needed to complete the daily cartfill process, which are all patient specific doses that are not loaded as common stock medications in the ADCs. A secondary objective was to reduce the amount of time involved in restocking of common stock medications in the ADCs on a daily basis by the pharmacy technicians.
Methods: Pharmacy automation analysts are members of the pharmacy informatics team, primarily responsible for maintenance of the cabinets, par and stock adjustments, and report writing. The analysts were able to evaluate specific canned reports to draft velocity reports, showing which ADCs possessed medications not being utilized effectively and which ADCs were missing medications as common stock items that were being routinely added and dispensed as a patient specific dose medication. Par levels for each drug added to the ADCs were adjusted as space allowed to account for package sizes stored centrally in pharmacy and to require an ADC restock no more than twice weekly. Velocity reports were run for the adult inpatient locations in the medical center, not including the emergency room or procedural area ADCs. This included a total of 104 ADCs reviewed. Common stock medications and associated par levels were added or adjusted in the ADC database starting in November 2016 and completed in March 2017.
Results: Of the 104 ADCs analyzed, the common stack rate of medications pulled increased from 85.4% in November to 86% in March, resulting in about a 0.5% increase in the rate of dispenses classified as common stock. The number of patient specific dispenses in every month went from 1,828 in November 2016, up to 1,936 in January 2017, and back down to 1,866 in March. Additionally, the number of restock transactions generated monthly for the ADCs went from 11,903 in November 2016, to 12,362 in January 2017, and then down to 11,602 transactions in February.
Conclusions: The results of the optimization efforts during the project did not show significant changes overall in the metrics identified. This 5 month longitudinal process was not robust enough to improve the percentage of common stock dispensing, reduce the number of patient specific dispenses from the ADCs, or reduce the number of medication restock transactions generated from the storage carousels. Efforts to optimize the ADCs through other means (par vs. utilization reports, ordered medications without removals, etc.) will be reviewed by the pharmacy automation team to ensure an ongoing, proactive approach to improving the use of the ADCs.
Submitting Author: Anthony Scott, PharmD
Organization: The University of Chicago Medicine
Authors: Kevin Colgan, MA, FASHP, Vice President, Chief Pharmacy Officer, The University of Chicago Medicine; Anthony C. Scott, PharmD, Assistant Director of Pharmacy Operations, The University of Chicago Medicine; Monika K. Lach, PharmD, PGY-1/PGY-2 Health-System Pharmacy Administration Resident, The University of Chicago Medicine; Bernice Y. Man, PharmD, PGY-2 Health-System Pharmacy Administration Resident, The University of Chicago Medicine.
ICHP
Poster Presentations – Original 3
(presented as Poster #11)
Category: Original-Research in Progress
Title: Medication Utilization and Patient Falls Correlated with the Use of Melatonin and Zolpidem in the Hospital
Purpose: Patient falls is one of the most common adverse events reported in the inpatient care settings. Among hospitalized patients, rates of falls range from 1.97 to 8.40 falls per 1000 patient-days. Patient falls prolong hospitalization, increase cost of care, and have the potential to cause serious injury. There are multiple risk factors reported in literature that are associated with falls, including: advanced age, muscle weakness, gait or balance problems, visual impairment, dizziness or vertigo, cognitive deficits, and use of psychotropic medications. Zolpidem is among one of the psychotropic medications commonly used in the inpatient setting that has been reported to decrease balance and has been independently associated with falls. Zolpidem use in hospitalized patients may be a potentially modifiable risk factor for falling. At University of Chicago Medicine (UCM), melatonin, an alternative sleep aide was added to the formulary in 2014. This project aims to compare falls that correlated with the use of zolpidem and melatonin as well as to analyze the prescribing pattern of zolpidem and melatonin at UCM since the addition of melatonin to formulary.
Methods: A retrospective analysis was conducted using data collected from patients between July and December of 2014 and July and December of 2015, which were defined as periods pre and post addition of melatonin to formulary respectively. Patients included in the study were greater than 18 years of age who received either zolpidem or melatonin or fell during the study time periods. Patients were identified by either having an adverse event report submitted for a fall and/or if they had an active medication order for either melatonin or zolpidem on pharmacy utilization reports.. Patients were excluded if they fell during an outpatient visit or if the location of the fall could not be determined due to incomplete reporting. The primary objective was to compare the incidence of falls in patients receiving melatonin or zolpidem, or both agents, or neither agent. The secondary objective was to analyze the utilization trends of zolpidem and melatonin at UCM during the study period. The following data will be collected: age, gender, date of patient fall, admitting service, hospital unit, days of sleep aide therapy, dosage and proximity of the last dose to the fall.
Results: Research in Progress. To be presented at meeting.
Conclusions: Research in Progress. To be presented at meeting.
Submitting Author: Lida Thimothy, PharmD, BCPS
Organization: University of Chicago Medical Center
Authors: Lida Thimothy, PhamD, BCPS, Clinical Pharmacist, University of Chicago Medical Center; Hailey Soni, PharmD, BCPS, Clinical Pharmacy Specialist - Internal Medicine, University of Chicago Medical Center; Judy Doty, MSN, RN, Nursing Quality Manager, University of Chicago Medical Center; Meghan Conroy Sweis, MSN, RN, Nursing Quality Specialist, University of Chicago Medical Center; Randall Knoebel, PharmD, BCOP, Clinical Manager, University of Chicago Medical Center.
***********************************************************************************
ICHP Poster Presentations – Original 4
(presented as Poster #28)
Category: Original-Research in Progress
Title: Most Valuable Components of Residency Training at the University of Chicago Medicine
Poster not presented.
****************************************************************************************
ICHP Poster Presentations – Original 5
Winner: Best Original Poster Presentation 2017
(presented as Poster #30)
Category: Original-Research in Progress
Title: Management of Heparin Infusions in
the Obese Population
Purpose: An update to the heparin infusion protocol
for the treatment of venous thromboembolism was implemented in a community
hospital. The objective was to review
the effects of using adjusted body weight (AdjBW) for patients weighing >150
kg.
Methods: This was a retrospective quality improvement project. Obese patients who were prescribed heparin were divided into three groups: 100-119 kg, 120-149 kg, and ≥150 kg. Inclusion criteria included documentation of a bolus and initial infusion and ≥2 PTT results. The primary outcome was time to first therapeutic PTT. Secondary outcomes included median initial PTT, median PTT at 24 hours, and bleeding episodes.
Results: The median times to therapeutic range for the 100-119 kg, 120-149 kg, and > 150 kg groups were 21 hours (IQR 13-25 h), 22 h (IQR 18-24 h), and 6 h (IQR 6-16 h) respectively. Therapeutic range was 65-104 seconds. At first PTT draw, the median PTT was 171 seconds (IQR 116-215 s), 186 s (IQR 117-260 s), and 77 s (IQR 65-92 s) and at 24 hours after the start of the infusion the median PTT was 83 s (IQR 70-112), 95 s (IQR 82-108), and 60 s (IQR 51-76 s) respectively.
Conclusions: The use of AdjBW for heparin boluses and initial infusion rates in patients weighing > 150 kg shortened time to therapeutic range compared to patients weighing 100-150 kg. However, these patients required several upward titrations to maintain therapeutic PTTs at 24 hours. Patients weighing 100-150 kg achieved highly supratherapeutic anticoagulation and required several downward titrations to achieve therapeutic range at 24 hours. Use of BMI in place of an actual body weigh cut-off for identifying patients at risk of over anticoagulation with standard heparin doses should be investigated.
Submitting Author: Kathryn Wdowiarz, PharmD, BCPS
Organization: Midwestern University and Edward Elmhurst Healthcare
Authors: Kathryn Wdowiarz, PharmD, BCPS, Assistant Professor, Midwestern University Chicago College of Pharmacy, Downers Grove, IL, and Internal Medicine Clinical Pharmacist, Edward Elmhurst Healthcare, Naperville, I; Danielle Petric, PharmD Candidate, Midwestern University Chicago College of Pharmacy, Downers Grove, IL.
ICHP Poster Presentations – Encore 1
(presented as Poster #13)
Category: Encore
Title: Evaluation of Sustained Virologic Response Rates after Hepatitis C Virus Treatment among a Diverse Patient Population at an Urban Academic Medical Center
Poster not presented.
***************************************************************************************
ICHP Poster Presentation – Encore 2
Winner: Best Encore Poster Presentation 2017
(presented as Poster #34)
Category: Encore
Title: Pharmacy Desensitization in a Collaborative Practice with Allergy Clinic
Purpose: Purpose: Desensitization is a medical treatment for some types of allergies with the aim to induce or restore tolerance to the allergen by reducing its tendency to induce IgE antibody production. Patients are desensitized through the administration of escalating doses of allergen that gradually decreases the IgE-dominated response. The purpose of this poster is to summarize and describe a model for an ambulatory care pharmacy to prepare, label and provide all desensitization medication needs to the Allergy clinic for patient specific administration.
Methods: Patient is seen at the Medical Center and is diagnosed with a disease state that requires the patient to use a drug they may be allergic to. For example, a patient may have a documented metronidazole allergy, but needs the drug for treatment of their diagnosed condition. The Allergy Clinic doctors become involved in the case and will enter a desensitization prescription for the patient. This prescription is sent to the outpatient pharmacy with a time and date that the order is needed by. The outpatient pharmacy assesses the appropriateness of the order by conducting a detailed clinical review, checking the compatibility and stability of products, as well as dosing calculations. Once all clinical requirements are met, the outpatient pharmacy also ensures the products are available and can be ordered through the pharmacy ordering system. With everything in place, the order is prepared and the Allergy Clinic staff picks up the order to administer to the patient in the clinic.
Results: This full-circle collaboration between an outpatient pharmacy and clinic staff allows for a mechanism of completing desensitization orders and ensuring delivery to the Allergy Clinic for the most effective patient care. It was determined that the outpatient pharmacy was best equipped to provide the desensitization orders to the Allergy Clinic because of the detailed clinical review provided, ability to order required products directly, as well as use of an on-site clean room. The outpatient pharmacy has an agreement with the Allergy clinic to have all orders prepared in time for the clinic staff to pick up and take back to clinic. Overall, a model of an outpatient pharmacy-prepared desensitization order was designed and implemented successfully for an affiliated Allergy Clinic. Specifically, patients that were noted to have a documented allergy were able to successfully undergo treatment for their medical condition without increased risk to their health.
Conclusions: An outpatient pharmacy staffed with pharmacists providing thorough clinical review of all desensitization orders and equipped with a sterile compounding facility is best suited to meet the needs for preparation of desensitization orders. All desensitization orders were prepared in a timely and efficient manner, allowing for patient access to quality care and further contributing to positive outcomes such as decreasing risk of allergic reaction during treatment, avoiding major side effects to medications, and decreasing cost for this sensitive patient population.
Submitting Author: Daniel Haywood, PharmD Candidate
Organization: University of Illinois Hospital & Health Sciences System, EEI Ambulatory Care Pharmacy
Authors: Sami Labib, RPh, Clinical Assistant Professor, Pharmacy Practice Assistant Director, Clinical Instructor. Monazzah Sarwar, PharmD, Clinical Instructor, Clinical Pharmacist; Steven Menachof, PharmD Candidate, EEI Extern; Daniel Haywood, PharmD Candidate, EEI Extern.
*****************************************************************************************
(presented as Poster #18)
Category: Student-Research in Progress
Title: The Deprescribing Conversation Project: Giving Nurses the “Words”
Purpose: With the growth of the older adult population in the United States, healthcare professionals are increasingly involved in end-of-life care across a multitude of practice settings including hospitals, skilled nursing facilities, home care, and hospices. Nurses typically are front line providers for patients nearing the end of life and are often expected to deliver precise communication regarding futile treatments and unnecessary medications to patients and families. These conversations can be challenging for nurses as well as emotional for patients and families, who find it difficult to understand why a medication once perceived as beneficial is now being discontinued. Pharmacists with their unique knowledge of pharmacotherapy including medication time-to-benefit (i.e. for statins and other preventive agents) and medication risk-to-benefit profiles may be able to provide nurses with the “words” for difficult deprescribing conversations. The purpose of this “Deprescribing Conversation Project” is to enhance hospice nurses’ knowledge and comfort with deprescribing conversations by providing a structured dialogue for discussing the benefits and burdens of drug therapy in patients with limited life expectancies.
Methods: Two patient-nurse vignettes were scripted and filmed using student pharmacist actors. Each scenario represents a common deprescribing situation; the first video depicts a conversation about discontinuing cholinesterase inhibitor therapy in a patient with late stage dementia. The second video depicts a conversation regarding inhaler polypharmacy in a patient with advanced pulmonary disease and diminished inspiratory capability. Each video illustrates a rational, patient-centered conversation about medication risk and benefit in the context of the patient's goals and life expectancy. With tactful and empathetic communication, the student pharmacist actor also addresses patient and family concerns as well as misconceptions. Registered hospice nurses in northern Illinois will be recruited to participate in viewing these two videos via email correspondence. Before and after viewing the videos, the study participants will be asked to complete a pre and post-survey to assess their perspective and knowledge of deprescribing and their comfort level with conducting these conversations. Pre-survey results will be compared to post-survey results to assess whether the filmed vignettes improved nurses’ knowledge and comfort with deprescribing conversations.
Results: Research in Progress. To be presented at meeting.
Conclusions: Research in Progress. To be presented at meeting.
Submitting Author: Patrice Davis, PharmD Candidate
Organization: University of Illinois at Chicago (UIC) College of Pharmacy at Rockford
Authors: Patrice Davis, PharmD Candidate, UIC College of Pharmacy at Rockford; Hans Scheerenberger, PharmD Candidate, UIC College of Pharmacy at Rockford; Laura Meyer-Junco, PharmD, BCPS, CPE, UIC College of Pharmacy at Rockford.
***************************************************************************************
ICHP Poster Presentation – Student 2
Winner: Best Student Poster Presentation 2017
(presented as Poster #36)
Category: Student-Research in Progress
Title: Reducing Polypharmacy: Deprescribing at an Academic Medical Center
Purpose: Polypharmacy is a growing problem within the healthcare system contributing to an increased risk of adverse drug reactions, potential drug-drug interactions, non-adherence to medications, and associated health care costs. The objective of this study is to reduce polypharmacy through the process of deprescribing. Deprescribing is defined as the process of tapering, stopping, discontinuing, or withdrawing drugs that are deemed inappropriate or no longer necessary. Deprescribing aims to manage polypharmacy and improve patient outcomes; therefore, reducing the risks associated with using multiple medications. Additionally, this study aims to enhance the standard of care by evaluating a patient’s home medication list during an inpatient hospitalization with the overall goal of simplifying the patient’s drug regimen.
Methods: This project was conducted in conjunction with a deprescribing quality improvement initiative at an academic medical center in Springfield, IL. The quality improvement team identified patients aged 65 years or older, taking at least 8 medications at home who were admitted to the Southern Illinois University (SIU) Internal Medicine Team and were patients at the SIU Internal Medicine Team Clinic. The patient’s home medication list was reviewed upon admission to the hospital by a pharmacist or a physician on the quality improvement team and potential unnecessary or inappropriate medications were identified with the intent of deprescribing. Stopping these medications was discussed with the patient and documented within their electronic health record. This study used a retrospective chart review to determine which home medications upon admission were considered inappropriate and eligible to be stopped and which medications were actually stopped. The study also recorded the physician rationale for why a particular medication was deprescribed.
Results: Of the numerous patients screened, 31 were eligible for this study. Of these eligible patients, the average number of medications upon admission and discharge was 16 and 15, respectively. On average, 3 medications were deprescribed per patient, yet 5 or more medications were discontinued in 26% of patients. The medications discontinued varied widely from antihypertensive agents, antiplatelet medications, antibiotics, and proton pump inhibitors amongst several other pharmacologic classes. In 45% of patients, the rationale for discontinuation of at least one medication was noted as unnecessary medication therapy and occasionally, the medication was responsible for the patient’s hospitalization.
Conclusions: Polypharmacy is a prominent issue in patients 65 years and older. These patients are on several medications, often unnecessarily. The process of deprescribing has several different challenges, but this initiative demonstrated the positive impact of simplifying a patient’s drug profile and it would be beneficial if such research was conducted on a larger scale.
Submitting Author: Morgan Atwood, PharmD Candidate
Organization: Southern Illinois University Edwardsville School of Pharmacy
Authors: N/A
*****************************************************************************************
ICHP
Poster Presentation – Student 3
(presented as Poster #39)
Category: Student-Research in Progress
Title: Fall Risk Assessments in a Community-based Senior Outreach Program
Purpose: Falls among older adults are a serious public health concern. Each year, one in three Americans 65 years and older falls. Of those falls, 55 percent lead to an unintentional injury or death. Medications are a modifiable risk factor for falls; therefore, screening for high-risk drug therapies plays a key role in mitigating medications' impact on falls risk. Furthermore, nationally recognized resources, tools and evidence-based falls prevention programs, exist to empower older adults to decrease their risk of falls. The aim of this study was to screen community based older adults for fall risk, promote community based Matter of Balance program (MOB), and refer those taking high-risk medications to comprehensive medication review (CMR).
Methods: Older adults were screened for fall risk in September 2016, predominantly, at local senior centers (n=15) and one Senior Fest. Assessments included: CDC STEADI Fall Risk Checklist (high risk: if answered Yes to 4 or more questions, if fallen in the past year, if taking medications for sleep or mood disorders, and/or if experiencing dizziness or fatigue due to medications), Timed Up and Go (TUG) test (high risk: >12 seconds), orthostatic blood pressure, and high risk medication class review. All older adults were encouraged to participate in MOB, and those taking high-risk medications were encouraged to have health care provided CMR. Program evaluation was assessed.
Results: Four hundred thirty nine participants (mean age 72.9, range 47-95) were assessed for fall risk. When permitted, those identified at higher risk of falls via the CDC STEADI tool (244/439, 55.58%) were further assessed. Reasons identified for fall risk included: TUG test (69/244, 28.28%), orthostatic blood pressure (11/244, 4.51%), and high-risk medications (150/244, 61.48%). High-risk medication classes included: CNS active medications- benzodiazepines, antipsychotics, anti-epileptics, antidepressants, sedatives, anti-parkinsons’, opioids, muscle relaxants and/or antihistamines (52/244, 21.31%), antihypertensives (126/244, 51.64%), and sulfonylureas (17/244, 6.97%). Older adults with two or more CNS active medications (20/244, 8.2%). Older adults likely to participate in CMR (163/439, 37.13%), MOB (169/439, 38.5%) and/or make changes to their home environment (153/439, 34.85%) as a result of the program were referred.
Conclusions: Fall risk assessments by health care providers in community based older adults accompanied with referral to structured evidence based medication reviews and self-care training programs contributes to overall public health, safety promotion and national fall prevention efforts.
Submitting Author: Yesha Patel, PharmD Candidate
Organization: University of Illinois at Chicago College of Pharmacy
Authors: Yesha Y. Patel, PharmD Candidate 2017, University of Illinois at Chicago College of Pharmacy, Hospital Pharmacy Extern, University of Illinois Hospital and Health Sciences System; Michael J. Koronkowski, PharmD, Clinical Assistant Professor, Department of Pharmacy Practice, University of Illinois at Chicago College of Pharmacy; Adam Bursua, PharmD, Clinical Assistant Professor, Department of Pharmacy Practice, University of Illinois at Chicago College of Pharmacy; Kristen L. Goliak, PharmD, Clinical Associate Professor, Department of Pharmacy Practice, University of Illinois at Chicago College of Pharmacy.
*****************************************************************************************
ICHP
Poster Presentation – Student 4
(presented as Poster #41)
Category: Student-Research in Progress
Title: Dose Adjustments of Thiopurines in Patients Based on Thiopurine Methyltransferase Activity
Purpose: Azathioprine is a prodrug whose active metabolite, 6-mercaptopurine (6-MP), is a purine analogue that exerts its immunosuppressive effects by interfering with DNA synthesis and repair. 6-MP is metabolized by the enzyme thiopurine methyltransferase (TPMT) to produce 6-methylmercaptopurine (6-MMP). Deficiency of this enzyme leads to excessive amounts of 6-MP, which then causes the metabolism to occur down an alternate pathway. This can result in life-threatening myelosuppression. TPMT is a cytoplasmic transmethylase that is present in most bodily tissues such as the heart, placenta, pancreas, intestine, and red blood cells. When using standard dosing, low levels of TPMT activity have been associated with an increased risk for thiopurine toxicities such as severe myelosuppression. Conversely, high activity levels have been associated with suboptimal treatment. Several studies have examined whether there is a benefit to testing markers of TPMT activity prior to the administration of thiopurines to guide empiric dosing adjustments. Currently, University of Chicago Medicine does not have a protocol that addresses specific starting doses and subsequent dose adjustments of thiopurines based on TPMT phenotype category. The purpose of this retrospective single center study is to identify optimal dosing for patients based on their TPMT phenotype category.
Methods: A lab report of all TPMT results from 1/1/2015 to 6/30/2016 will be used to identify patients that received phenotype testing. Additional data will be obtained from the electronic medical record, including patient demographics and baseline characteristics [age, sex, race, CrCl, TPMT phenotype category (low, low normal, normal, or high), indication for treatment, specific thiopurine drug utilized, initial thiopurine dose, CBC, AST, ALT, alkaline phosphatase, bilirubin, number of subsequent dose adjustments, and final dose]. The primary endpoint will be the final dose for each TPMT phenotype category. Secondary endpoints are the percentage of patients that received dose adjustments based on TPMT phenotype category, the average number of dose adjustments, and the percentage of patients who experiences toxicities and adverse events. Inclusion Criteria: •All patients at UCM who received TPMT phenotype testing between January 1, 2015 and June 30 2016 Exclusion Criteria: •Patients who received no doses of thiopurine drugs following TPMT testing •Pregnant and lactating women •Patients taking febuxostat, doxorubicin, or allopurinol at the time of thiopurine initiation •Patients with a blood transfusion within 60 days prior to TPMT testing •History of use of alkylating agents: Altretamine, Bendamustine, Busulfan, Carboplatin, Carmustine, Chlorambucil, Cisplatin, Cyclophosphamide, Estramustine, Ifosfamide, Lomustine, Mechlorethamine, Melphalan, Oxaliplatin, Procarbazine, Streptozocin, Thiotepa, Dacarbazine, Temozolomide •Renal transplant rejections •Renal impairment, defined as CrCl <50 ml/min, or patients on Hemodialysis or Continuous Renal Replacement Therapy Statistical Analysis: •Descriptive Statistics •Multi-variant logistic regression
Results: Research in Progress. To be presented at meeting.
Conclusions: Research in Progress. To be presented at meeting.
Submitting Author: Brittany Huff, PharmD Candidate
Organization: University of Chicago Medical Center
Authors: Brittany M Huff, PharmD Candidate, Chicago State University College of Pharmacy, Student Pharmacist; Trevor N. Christ, PharmD, University of Chicago Medical Center, Clinical Pharmacy Specialist-Adult Hematology/Oncology; Shannon M. Rotolo, PharmD, BCPS, University of Chicago Medical Center, Clinical Pharmacy Specialist-General Pediatrics.
*************************************************************************************
ICHP Poster Presentation – Student 5
(presented as Poster #42)
Category: Student-Research in Progress
Title: The Impact of Pharmacist-Driven Pantoprazole to Famotidine Substitution Protocol on Rates of Hospital-Acquired Clostridium difficile
Poster not presented.
*********************************************************************************************
ICHP Poster Presentation – Student 6
(presented as Poster #43)
Category: Student-Research in Progress
Title: Evaluation of Pain Medication Management in Patients Admitted to a Large Academic Hospital
Poster not presented.
*********************************************************************************************
Board of Pharmacy Update
Highlights of the March Board of Pharmacy Meeting
by Scott A. Meyers, Executive Vice President
The March 14th Board of Pharmacy Meeting was held at the Illinois Department of Financial and Professional Regulations offices in Springfield. These are the highlights of that meeting.
Practice Act Sunset – The Department is running two identical bills that will update the Pharmacy Practice Act Sunset date and a few other changes. The bills, SB0902 sponsored by Sen. Dale Righter, R-Mattoon and HB3462 sponsored by Rep. Mike Zalewski, D-Riverside would extend the effective date of the Act through Dec. 31, 2027 and would also make a few minor changes including requirement of email addresses for each registrant or applicant, removal of State Board of Pharmacy member per diems, deletion of the minimum required number of pharmacy inspectors and deletion of the position of deputy pharmacy compliance coordinator.
Affiliated Monitors – Beth Anne Compton, JD, Regional Director of Affiliated Monitors presented an overview of their company and services that could be used by pharmacies or pharmacists who have been court ordered independent monitors as a condition of a discipline against their licenses. The company already works with the Illinois Medical Board as an independent monitor of physicians who have received discipline of some sort and are now required to provide regular reports from an independent monitor. Situations like Medicare fraud, insurance fraud, diversion or other violations often require an outside company to provide reports to the Board. Affiliated Monitors currently provide services to individual clients (not the State agencies, medical boards or pharmacy boards) in 27 State and have live cases where they monitor individuals practices defined by court order for five State Boards of Pharmacy in Rhode Island, New Jersey, Tennessee, Colorado and Nevada. They have provided pharmacy monitoring services in Texas and Iowa in the past. They work for and are paid by the disciplined individual but report to the respective medical or pharmacy board of that State. The presentation was informational so that the Board and Department staff are familiar with their services.
2017 License Renewals – Chances are this article will be published in April, and the deadline for 2017 license renewals will be past (March 31st). This year only pharmacy technicians’, certified pharmacy technicians’ and student pharmacists’ licenses are up for renewal. At the time of the Board meeting nearly two-thirds of the licensed individuals had still not renewed. ICHP sent out a reminder to its pharmacy director members in March reminding them to make sure their technicians renewed before the deadline.
Legislative Update – At each Board of Pharmacy meeting, ICHP or IPhA staff provide a summary of pharmacy-related legislation before the General Assembly. At this meeting a 23-page document was summarized by yours truly. While ICHP has over 80 bills and resolutions that it is currently monitoring, about 20 of these bills were discussed. A full report of bills before the General Assembly can be found in the Government Affairs Report in this issue of KeePosted.
Next Board of Pharmacy Meeting – The next meeting of the Illinois Board of Pharmacy will be held at 10:30 AM on Tuesday, May 9th at the James R. Thompson Center in downtown Chicago. Announcements and agendas are posted at least 14 days in advance on the IDFPR pharmacy website. The profession is welcome to attend the open portion of this meeting.
College Connection
Therapy Dog Thursday
College Connection
by Aprille Banchoencharoensuk, P2, ICHP Secretary, Rosalind Franklin University of Medicine and Science College of Pharmacy
As students in a graduate program, we often find ourselves stressed out with upcoming exams and deadlines. To cope with the stress, some students join intramural groups or others seek comfort from their family and friends. However, this can be difficult with a busy schedule or when home is thousands of miles away. There are others like myself who use a different outlet provided by our school - Therapy Dog Thursday.
Therapy Dog Thursday is an event that is organized by a Rosalind Franklin University of Medicine and Science’s (RFUMS) faculty, Beth Friedman. Once a month, Beth organizes the meetings with these cuddly pups from Our House of Hope Rescue. This rescue organization was founded in 2007 and is led by a wonderful woman, Lisa Krinninger, who is the Executive Director. Currently all of the dogs in this organization are living with foster families and are available for adoption. For a few hours that day, the dogs join us for a time filled with belly rubs and scratches behind the ear. Each visit we are always joined with new furry faces and once in a while, we get to meet the occasional rabbit. This organization also fosters and rehabilitates a variety of different animals such as gerbils, squirrels, and turtles. This program serves as a great way for these animals to socialize and to find prospective homes. It is also a great resource for animal lovers or those who find comfort in cute and fluffy four legged friends.
The first time I visited these pups, I was in my first year at RFUMS. I was still acclimating to graduate school life and was stressed out due to having to commute two and half hours every day to school. Therapy Dog Thursday fit right into my busy schedule, since it was offered on campus and during convenient hours around lunch. I was able to walk right over to the area where these pups sat during my break and instantly, I was untroubled with the stresses of school and commuting. All the dogs are so friendly and well behaved. I was met with wagging tails and lots of kisses. I sat there with the dogs and made my rounds to pet each one. I paid particular attention to a scruffy black dog that reminded me a lot of my cousin’s dog I grew up with, that recently passed away. I sat there for the remainder of the hour petting her and forgetting the laundry list of things I had to do. Fellow classmates and students from other professional programs joined me that day for the company of these sweet dogs. Therapy Dog Thursday is a great way to help students unwind and get away from our hectic schedules. Somehow, just a simple visit from these furry friends can uplift the spirit, which is why I choose to continue to stop by when I can.
I am currently in my second year in pharmacy school at RFUMS. I no longer have the stress of commuting since I have moved closer to campus, but school is still as hectic as the previous year. I stop by to visit the dogs whenever I can, even if it is for a few minutes. Since moving closer to campus, I have had to leave my own dog at home which gives me a lot more reason to continue to visit these dogs. This organization has helped me as well as countless other students and faculty by finding comfort in these friendly pups.
This program has been very well received since it began three years ago. A recent survey about the program was conducted and demonstrated positive impact on current and former students. Therapy Dog Thursday has been able to help brighten days, while helping us destress from school, and cope with missing our own furry babies waiting for us at home while we attend school. There is something soothing about visiting these animals which truly make them therapy dogs. I look forward to many more Therapy Dog Thursdays and I hope that other schools will consider adopting a similar program as well.
Developing Leadership, A Reflection
College Connection
by Lisa Nguyen, PS-3, ICHP-MWU Historian, Midwestern University Chicago College of Pharmacy
More
Upcoming Events

Thursday, April 13, 2017
Pharmacist Role in Hospice and Palliative Care
Chris Herndon, PharmD
West Central Society LIVE Program
Saint Francis Medical Center | Peoria, IL
Accredited for pharmacists and
pharmacy technicians | 1.0 contact hour (0.1 CEU)
Tuesday, May 9, 2017 - Save the Date
Combating the Opioid Epidemic Through SBIRT
Tran Tran, PharmD, BCPS
Champions
LIVE Webinar
Accredited for pharmacists and pharmacy technicians | 0.5
contact hours (0.05 CEU)
Save the date! Watch for
more information in upcoming news briefs.
Tuesday, May 9, 2017 - Save the Date
Pharmacist Role in Hospice and Palliative Care
Chris Herndon, PharmD
Sangamis Society LIVE Program
Accredited for pharmacists and pharmacy technicians |1.0 contact hour (0.1 CEU) Save the date! Watch for more information in upcoming news briefs.
Tuesday, May 18, 2017 - Save the Date
Crohn's Disease and Ulcerative Colitis: New Perspectives in Therapy
Cassandra Collins, PharmD
OSF Saint Francis Medical Center, Peoria
West Central Society LIVE Program
Save the date! Watch for more information in upcoming news briefs.
Thursday, June 15, 2017
Cultivating Safety in the Pharmacy
Adam Bursua, Pharm.D., BCPS
Champions LIVE Webinar for Pharmacy Technicians
Accredited for pharmacy
technicians and pharmacists | 0.5 contact hour (0.05 CEU)
Save the date! Watch for more information in
upcoming news briefs.
Saturday, July 1, 2017
2017 Best Practice Award Submissions Due
More information on the 2017 Best Practice Award and Program coming soon.
Leadership Profile
Lara K. Ellinger, PharmD, BCPS - Drug Information and Medication Safety Pharmacist, Northwestern Memorial Hospital

What is your current leadership position in ICHP?
Director of Educational Affairs
What benefits do you see in being active in a professional association such as ICHP?
Learning from and exchanging ideas with other like-minded pharmacists; being encouraged by colleagues to challenge myself; and working together to further the profession of pharmacy.
What initially motivated you to get involved in ICHP?
I liked the sense of community I felt at ICHP events and the idea of developing my pharmacy leadership skills outside of my work setting.
Where did you go to pharmacy school?
University of Illinois at Chicago College of Pharmacy (UIC)
Where have you trained and/or worked?
I completed a PGY-1 Pharmacy Residency at Northwestern Memorial Hospital (NMH) in Chicago and then completed a PGY-2 Drug Information Residency at UIC. After my PGY2, I began as a faculty member practicing in Drug Information at UIC, and currently I work in drug information and medication safety at NMH.
What special accomplishments have you achieved?
I think staying involved and active in my career and balancing my home life is a special accomplishment J
Describe your current area of practice and practice setting.
I work in a large academic medical center in downtown Chicago. I have a hybrid position that includes drug information, medication use policy, and medication safety. I respond to drug information requests from practitioners within the institution; prepare monographs and help coordinate P&T committees; serve as pharmacy lead for the Medication Safety P&T Committee; review medication errors and adverse events; and make process changes to prevent errors and facilitate creating a just culture in my department and institution overall. The best part of my job is collaborating with multiple departments (e.g., Risk, Quality, Performance Improvement) to implement changes that make our institution safer for patients.
Is there an individual you admire or look up to or a mentor that has influenced your career?
Desi Kotis for setting daily examples of leadership and leading me to numerous career-advancing opportunities; Joan Stachnik for endless support and reminders to stay balanced in life; Mike Gabay for instilling thoroughness and efficiency in all of my work; Amy Lodolce for treating me as a colleague when I was a resident; and Mike Fotis for encouraging me to always seek opportunities for involvement in the profession of pharmacy.
What advice would you give to student pharmacists?
Whatever you choose to do right after graduation, keep in mind that it’s actually not the most important decision despite it feeling that way sometimes! There are also multiple pathways to get to where you want to be. For most people, where they want to be is constantly evolving.
What pharmacy related issues keep you up at night?
Figuring out how I can best utilize residents and students to help me get projects done. I really can’t be effective in this position without them. It’s a win-win situation!
Do you have any special interests or hobbies outside of work?
Of course! They include hiking, skiing, crafting, and calligraphy.
Do you have a favorite restaurant or food?
I eat everything! A great place for steak is Bavette’s in Chicago. Although they don’t advertise it, you can bring in your own bottle(s) of wine, but their rule is you have to share a glass with someone else dining there. You can either choose who you give the glass to or the server can. The food is so good, I usually have to be rolled out of that place.
What is your favorite place to vacation?
Anywhere that has mountains
What is the most interesting/unique fact about yourself that few people know?
I’ve climbed and summited a few mountains!
What 3 adjectives would people use to best describe you?
Proactive, reliable, motivated
ICHP Pharmacy Action Fund (PAC) Contributors
 Save to PDF
Save to PDFRonald Miller
Officers and Board of Directors
815-599-6113
mweaver@fhn.org
LARA ELLINGER
Director, Educational Affairs
laelling@nm.org
KRISTI STICE
Director, Professional Affairs
kristi.stice@hshs.org
816-885-4649
david.tjhio@bd.com
JACOB GETTIG
Editor & Chairman, KeePosted Committee
630-515-7324 fax: 630-515-6958
jgetti@midwestern.edu
Assistant Editor, KeePosted
630-515-7167
jphillips@midwestern.edu
Executive Vice President, ICHP Office
815-227-9292
scottm@ichpnet.org
Regional Director North
Regional Co-Director South
President, Student Chapter
Chicago State University C.O.P.
sbarkat14@midwestern.edu
President, Student Chapter
Roosevelt University C.O.P.
JORIE KREITMAN
President, Student Chapter
Rosalind Franklin University C.O.P.
jorie.kreitman@my.rfums.org
President, Student Chapter
Southern Illinois University Edwardsville S.O.P
mabelch@siue.edu
ICHP Affiliates
ANTOINE JENKINS
President, Northern IL Society (NISHP)
JARED SHELEY
President, Metro East Society (MESHP)
KATELYN CONKLEN
President, Sangamiss Society
ED RAINVILLE
President, West Central Society (WSHP)
ed.c.rainville@osfhealthcare.org
Vacant Roles at Affiliates —
President, Rock Valley Society; Southern IL Society; Sugar Creek Society
Welcome New Members!
| New Member | Recruiter |
| Mohammed Alchaar | Lauren Stambolic |
| Angela Barnes | |
| Jacqueline Barraclough | |
| Mike Bolanos | |
| Melissa Bonacquisti | |
| Todd Branson | Ken Ring |
| Toni Burke | |
| Patricia Cantieri | |
| Ashley Cha | Lauren Stambolic |
| Benjamin Chong | |
| Teresa Colvin | |
| Deb Egerere | |
| Lauren Ellis | |
| Nicole Ewald | |
| Michelle Fine | |
| Ernestine Foster | Jan Keresztes |
| Tomas Garbaliauskas | |
| Paloma Garcia | Katarzyna Plis |
| Sheila Grasso | |
| Michele Hentcheu | |
| Genie Lil Herrera | Darina McDee |
| Serin Homsi | Lauren Stambolic |
| Deborah Jafraty | |
| Don Janczak | |
| Holly Jones | Cheryl Scantlen |
| Taylor Jones | |
| Theodora Jurichko | |
| Katie Kaczmarski | |
| Amir Kagdi | |
| Jennifer Karp | Jo Ann Haley |
| Beverly Kenny | |
| Kristina Laurente | |
| Amy Lee | |
| Pohung Lin | |
| Christine Lydon | Lauren Stambolic |
| Anna Majerczak | Katarzyna Plis |
| Katrina Marquez | |
| Nichele Marquis | Matthew Vogel |
| Doug Moon | |
| Victoria Nguyen | |
| Darlene Nicoloff | |
| Selina Nokes | |
| Kara Ozee | Kristi Stice |
| Tuyen Pham | Yuxiang Ou |
| Kenneth Ring | |
| Christy Roe | |
| Drazen Savic | Michelle Jeong |
| Paul Stranges | |
| Alaa Sulh | Katarzyna Plis |
| Leke Sylaj | |
| Patrick Tednes | |
| Scott Tyler | |
| Adam Wahab | |
| Dyson Wake | Henry Dunnenberger |
| Hannah Wake | Henry Dunnenberger |
| Asha Yusuf Save to PDF |