Print Entire Issue
_web578x100.png)
KeePosted Info
Features
Call for Entries: 2015 Best Practice Award
2015 Annual Meeting Registration Now Open!
Call for 2016 Nominations
ICHP Pharmacy Technician of the Year Award
ICHP Teams Up with Little By Little
Family Night at the Ballpark
Special Announcement - CPRN Collaborative Research Project
Columns
President's Message
Directly Speaking
New Practitioners Network
Leadership Profile
Government Affairs
Professional Affairs
Educational Affairs
Board of Pharmacy Update
College Connections
Pharmacists’ Evolving Role in Diabetes Management
Philanthropic Opportunities
Student-Faculty Networking Social
More
Welcome New Members!
Officers and Board of Directors
Upcoming Events
KeePosted Info
Illinois Council of Health-System Pharmacists
4055 North Perryville Road
Loves Park, IL 61111-8653
Phone: (815) 227-9292
Fax: (815) 227-9294
www.ichpnet.org
KeePosted
Official Newsjournal of the Illinois Council of Health-System Pharmacists
EDITOR
Jacob Gettig
ASSISTANT EDITOR
Jennifer Phillips
MANAGING EDITOR
Scott Meyers
ASSISTANT MANAGING EDITOR
Trish Wegner
DESIGN EDITOR
Amanda Wolff
INTERIM DESIGN EDITOR
Brittany Reuber
ICHP Staff
EXECUTIVE VICE PRESIDENT
Scott Meyers
VICE PRESIDENT - PROFESSIONAL SERVICES
Trish Wegner
DIRECTOR OF OPERATIONS
Maggie Allen
INFORMATION SPECIALIST
Heidi Sunday
CUSTOMER SERVICE AND
PHARMACY TECH TOPICS™ SPECIALIST
Jo Ann Haley
ACCOUNTANT
Jan Mark
COMMUNICATIONS MANAGER
Amanda Wolff
INTERIM COMMUNICATIONS MANAGERBrittany Reuber
LEGISLATIVE CONSULTANT
Jim Owen
ICHP Mission Statement
Advancing Excellence in the Practice of Pharmacy
ICHP Vision Statement
ICHP dedicates itself to achieving a vision of pharmacy practice where:
- Pharmacists are universally recognized as health care professionals and essential providers of health care services.
- Patients are aware of the training, skills, and abilities of a pharmacist and the fundamental role that pharmacists play in optimizing medication therapy.
- Formally educated, appropriately trained, and PTCB certified pharmacy technicians manage the medication distribution process with appropriate pharmacist oversight.
- Pharmacists improve patient care and medication safety through the development of effective public policies by interacting and collaborating with patients, other health care professionals and their respective professional societies, government agencies, employers and other concerned parties.
- Evidence-based practices are used to achieve safe and effective medication therapies.
- There are an adequate number of qualified pharmacy leaders within the pharmacy profession.
- Pharmacists take primary responsibility for educating pharmacy technicians, pharmacy students, pharmacist peers, other health professionals, and patients about appropriate medication use.
KeePosted Vision
As an integral publication of the Illinois Council of Health-System Pharmacists, the KeePosted newsjournal will reflect its mission and goals. In conjunction with those goals, KeePosted will provide timely information that meets the changing professional and personal needs of Illinois pharmacists and technicians, and maintain high publication standards.
KeePosted is an official publication of, and is copyrighted by, the Illinois Council of Health-System Pharmacists (ICHP). KeePosted is published 10 times a year. ICHP members received KeePosted as a member benefit. All articles published herein represent the opinions of the authors and do not reflect the policy of the ICHP or the authors’ institutions unless specified. Advertising inquiries can be directed to ICHP office at the address listed above. Image disclaimer: The image used in the Pharmacy Tech Topics™ advertisement is the property of © 2015 Thinkstock, a division of Getty Images.
Copyright © 2015, Illinois Council of Health-System Pharmacists. All rights reserved.
Features
Call for Entries: 2015 Best Practice Award

The objective of the Best Practice Award program is to encourage the development of innovative or creative pharmacy practice programs or innovative approaches to existing pharmacy practice challenges in health systems within the state of Illinois.
Applicants will be judged on their descriptions of programs and practices employed in their health system based on the following criteria:
- Innovativeness / originality
- Contribution to improving patient care
- Contribution to institution and pharmacy practice
- Scope of project
- Quality of submission
If you have any questions related to the program please contact Trish Wegner at trishw@ichpnet.org.
Previous Winners
2014
Arti Phatak, Pharm.D.; Brooke Ward, Pharm.D., BCPS; Rachael Prusi, Pharm.D.; Elizabeth Vetter, Pharm.D.; Michael Postelnick, BS Pharm, BCPS (AQ Infectious Diseases); and Noelle Chapman, Pharm.D., BCPS
“Impact of Pharmacist Involvement in the Transitional Care of High-Risk Patients through Medication Reconciliation, Medication Education, and Post-Discharge Callbacks”
2013
Nicole Rabs, Pharm.D., Sarah M. Wieczorkiewicz, Pharm.D., BCPS, Michael Costello, PhD, and Ina Zamfirova, BA
“Development of a Urinary-Specific Antibiogram for Gram Negative Isolates: Impact of Patient Risk Factors on Susceptibility”
2012
Kathryn Schiavo, Pharm.D.; George Carro RPh, MS, BCO; Abigail Harper, PharmD, BCOP; Betty Fang, PharmD; Palak Nanavati, PharmD
“Outpatient Oncology Treatment Center Approach to Enhancing Continuity of Care Related to Dispensing Oral Chemotherapeutic Agents”
2011
Fatima Ali, PharmD; Sarah Wieczorkiewicz, PharmD, BCPS; Jill Cwik, PharmD; Robert Citronberg, MD, FACP, FIDSA
“Procalcitonin-Guided Duration of Antimicrobial Therapy for the Treatment of Lower Respiratory Tract Infections”
|
Online entry form: http://www.ichpnet.org/professional_practice/best_practices/
Submission deadline: July 1, 2015
Eligibility
Applicants must be a member of ICHP practicing in a health system setting. More than one program can be submitted by a health system for consideration. Past submissions may be re-submitted if not previously given the award. Any new data should be included.
Instructions for preparing manuscript
Each entry for the Best Practice Award must include a manuscript prepared as a Word document, double-spaced using Times New Roman 12-pitch type. A header with the paper title and page number should appear on each page. The manuscript should not exceed 2000 words in length (not counting references), plus no more than a total of 6 supplemental graphics (tables, graphs, pictures, etc.) that are relevant to the program. Each picture, graph, figure, and table should be mentioned in the text and prepared as a separate document clearly labeled.
The manuscript should be organized as a descriptive report using the following headings:
- Introduction, Purpose, and Goals of the program
- Description of the program
- Experience with and outcomes of the program
- Discussion of innovative aspects of programs and achievement of goals
- Conclusion
Format
Submissions will only be accepted via online submission form. The manuscript will be forwarded to a pre-defined set of reviewers. Please do not include the names of the authors or affiliations in the manuscript to preserve anonymity.
All applicants will be notified of their status within three weeks of the submission deadline. Should your program be chosen as the winner:
- The program will be featured at the ICHP Annual Meeting. You will need to prepare a poster to present your program and/or give a verbal presentation. Guidelines will be sent to the winner.
- You will be asked to electronically submit your manuscript to the ICHP KeePosted for publishing. This program will be accredited for CPE and will require that you complete material for ACPE accreditation.
- You will receive a complimentary registration to the ICHP Annual Meeting, recognition at the meeting and a monetary award distributed to your institution.
Non-winning submissions may also be considered for publication in the ICHP KeePosted, but your permission will be obtained beforehand.
Thank you to PharMEDium for providing a grant for the 2015 Best Practice Award!
|
2015 Annual Meeting Registration Now Open!

Have you ever dreamed of being a character in a play or movie? To be an integral part of creating a special and engaging environment for the audience? To feel like you are part of something special? Would you like to be a star? Well, you are already doing that – in a way. Each of us has a special role to play in taking care of our patients and collaborating with others in the healthcare team. You play a crucial part each day in establishing a safe and collegial atmosphere for patients and co-workers.
The presidential theme for ICHP this year is collaboration - working together to create positive outcomes. This theme is showcased in our Annual Meeting programming through playing our part in providing excellent patient care. Center stage is our primary keynote presentation by the team of Brian Cross, Pharm.D. and Reid Blackwelder, MD. They will tell the story of how this pharmacist-physician collaboration plays out at East Tennessee State University Family Medicine Clinics. A health care team - comprised of a nurse, physician, family medicine resident and medical students, pharmacist, pharmacy resident and pharmacy students - works collaboratively to establish better patient outcomes and create an “area of mutual respect”. Come learn from their model of team-based care, with improved reimbursement system and patient outcomes on Friday, September 11th. Other main scenes are the keynotes for Thursday and Saturday of the meeting bringing to light the issues of provider status, pharmacist and technician workforce issues, and USP 800. Don’t miss out on other acts – go through our meeting highlights to find out more.
There will be plenty of intermissions to network with the rest of the “audience”. Join us for the NPN Mixer Friday night after the educational sessions to meet new practitioners in Illinois. Students can enjoy some fun at the Party at the Pit also on Friday night at the Hilton Garden Inn. Everyone can participate and have a role in advancing services and initiatives within ICHP at the Town Hall during lunch on Friday. Contribute to the ICHP Political Action Committee by participating in the ring toss. See who does and does not have good hand-eye coordination. Lots of collaboration can take place in the exhibit hall Thursday and Friday, and at the Residency Showcase on Saturday.
Go ahead, be a star! Join the rest of the stars at the 2015 ICHP Annual Meeting.
Call for 2016 Nominations
How Would You Like To Run For An ICHP Office?
by Scott A. Meyers, Executive Vice President
Every year, ICHP elects new members to its Board of Directors. As existing officers complete their terms, they often move up to higher offices or move on for a variety of reasons, not the least being that they’ve completed the highest offices of President-elect, President and Immediate Past President. So every year the ICHP Committee on Nominations searches for new leaders to step up to carry on the business of the Council and who are dedicated to “Advancing Excellence in Pharmacy!” That’s ICHP’s recently revised mission by the way.
This year is no exception. With Mike Fotis completing his term as Immediate Past President, Travis Hunerdosse and Brandi Strader completing their final terms as Director of Educational Affairs and Chair of the New Practitioners Network, respectively, there are at least three offices for which ICHP will need at least two candidates to run each. In addition, Board members Charlene Hope, Mike Weaver, Carrie Vogler, and Ana Fernandez can run for another term for their respective offices and may or may not have yet committed. And even if they do decide to run again, the Committee on Nominations will be seeking a second candidate to fill the ballot completely.
Below is a list of the offices open for election in the fall of 2015. All the elected candidates will take office at the 2016 Annual Meeting with the exception of the President-elect, who assumes office immediately. So each new leader will have almost a year to train for their new jobs and be coached by our current Board members. You don’t have to run that office unprepared!
President-elect
Secretary-elect
Chair of the House
Director-elect of Division of Educational Affairs
Director-elect of the Division of Marketing Affairs
Technician Representative-elect
NPN Chair-elect
If you are interested in running for an office or you would like to know more about an office before committing to run, you may contact Committee on Nominations Chair, Mike Fotis at michael.fotis@northwestern.edu or Scott Meyers at scottm@ichpnet.org. We hope you are ready to run for the lead of ICHP and pharmacy!
ICHP Pharmacy Technician of the Year Award
ICHP, through the Division of Marketing Affairs, is pleased to announce the first annual Pharmacy Technician of the Year award! Please see the criteria and instructions below and consider nominating a deserving pharmacy technician with whom you work. The deadline for nominations is June 9, 2015.
Award Purpose: The ICHP Pharmacy Technician of the Year Award is established to identify and recognize exceptional performance by a certified pharmacy technician within the State of Illinois.
Award Criteria:
The candidate must:
· Be a current ICHP technician member
• Be a PTCB certified pharmacy technician for at least two years
• Demonstrate at least one of the following:
- exceptional contributions to his/her pharmacy worksite
- exceptional contributions to ICHP as a volunteer member
- exceptional contributions to the practice of pharmacy in Illinois
Nomination Process:
A call for nominations will be made in the March/April KeePosted each year. That announcement may be augmented with appropriate e-mail blasts.
The nominator must:
· Be the technician’s supervisor, colleague or co-worker. No self-nominations will be accepted.
• Provide the following information:
o Worksite name, address and telephone number.
o Technician name and year certified.
o Describe the technician’s contributions in detail.
o Provide the nomination to the ICHP office by no later than June 9th for 2015.
Selection Process:
· All nominations are reviewed by the Division of Marketing Affairs at their June conference call.
• The Division will select two finalists for consideration and present them to the ICHP Board of Directors at the July Board Meeting.
• The ICHP Board of Directors will select the award winner from the two finalists presented by the Division of Marketing Affairs.
• The Division of Marketing Affairs may recommend one of the two finalists by providing detailed discussion points to the Board of Directors.
• The Board is not required to select a recipient if no candidate seems qualified.
Award:
· The Award will be presented at the ICHP Annual Meeting in September, if a technician is selected.
• The Award recipient and her/his nominator will be notified immediately following his/her selection by the Board of Directors.
• The award recipient will receive a complimentary full registration to the ICHP Annual Meeting.
· The award recipient will receive a plaque to be presented at an appropriately agreed upon time during the ICHP Annual Meeting. The nominator will be invited to participate in the award ceremony.
To nominate someone for this award, please forward a detailed letter of recommendation identifying the specific accomplishments of the nominee with respect to each criteria above to: ICHP, 4055 N Perryville Road, Loves Park, IL 61111-8653, or email to
scottm@ichpnet.org.
ICHP Teams Up with Little By Little
Medical Missions to Haiti
by Scott A. Meyers, Executive Vice President
The Illinois Council of Health-System Pharmacists now has a new informal partner to make a small portion of the world a better place! Little by Little is a non-profit organization that faithfully partners with those in need of improved health and well-being. Little by Little has been organizing medical professionals and graduate level health professional students in service learning teams since 2006. Their teams provide primary health care at a rural clinic in Gramothe, a mountainous village approximately 15 miles from Port-au-Prince, the capital city of Haiti. Over the course of one week, their team examines and treats over 200 patients per day. Physicians, advanced practice nurses, pharmacists, registered nurses, pharmacy technicians, lab technicians and those dedicated to their pharmacy and supply inventory compile a typical team of 25-30 volunteers. By partnering with Mountain Top Ministries (MTM), a Haitian run organization that maintains the clinic and hires local clinic support staff and translators, we are able to capacity build with their resources and collaborate with other volunteer medical teams who also visit MTM throughout the year.
Little by Little brings teams to Gramothe in January, March, May, August and October each year. They still have openings for pharmacists on the August team (traveling 8/10-17, 2015) and the October team (traveling 10/12-19, 2015). The typical cost for the volunteer is broken down by airfare (ranging from $600-850), room and board and ground transportation ($500). A donation of $100 is made at the time of application, which pays for the volunteer’s group travel /emergency evacuation insurance and any incidentals the team might encounter while in Haiti.
Sustainability and reciprocity are the corner stones of Little by Little’s mission and vision. By faithfully partnering with those in need of improved health and well-being, together their medical volunteers can make a big difference, little by little.
The ICHP Executive Committee reviewed Little by Little’s program and has now placed a brief description of its program and a link to their website on the ICHP website at www.ichpnet.org on the
Community Service page. If you have ever wanted to participate in a medical mission, Little by Little might be a great place to start!
Family Night at the Ballpark

ICHP's Central Region is sponsoring a family night at the ballpark.
Springfield Sliders vs. West Virginia Miners
Thursday, July 16, 2015
Game Time 6:35 PM
Family Night at the Springfield Slider’s Game VIP Suite seating with catered meal and two drinks (soda or beer). Tickets are $21.50 for adults. Children 3 and under are free and we may have special pricing for children under 7 years of age. Registration deadline is July 2nd.
Robin Roberts Stadium at Lanphier Park
1415 North Grand Avenue
Springfield, IL 62702
Enjoy a summer game, camaraderie and great ball park food! All ICHP Central Region members are welcome. Since it is family night, you may purchase more than one ticket per person. You will need to register by calling the ICHP office at (815) 227-9292 to reserve tickets. Please state how many tickets and the ages of any children attending. The price of a ticket includes the game seating, meal and two drinks. Your credit card will be charged once all tickets are sold. Meeting new people and making friends will be priceless!
Tickets will be mailed to you once your order is processed. We look forward to cheering with you soon! Come enjoy this networking opportunity, and remember to bring your business cards. This is a great opportunity also for new residents in the area to get to know each other.
Special Announcement - CPRN Collaborative Research Project
The ICHP Clinical Practice and Research Network (CPRN) is pursuing the possibility of working on collaborative research projects in Illinois. If you have a research project idea you would like to initiate with participation from other healthcare institutions in order to increase its impact as multi-center research then send a brief overview (the study question and short description of the proposed methodology) of your research to Dr. Trish Wegner at trishw@ichpnet.org by July 20th for consideration. We will discuss proposals at the October CPRN meeting. The meeting will be via teleconference so that all IL institutions can participate.
Columns
 President's Message
President's Message
Welcoming a New Grad
by Linda Fred, ICHP President
Congratulations to the Class of 2015! My own daughter is among the happy recipients of college degrees this spring, and so we have been working on all the associated activities – ordering a cap and gown, sending out graduation announcements, planning a party. There is a lot of ‘hoopla’ around ending this chapter of the college student’s life. Our new graduates are also thinking about the next chapter – moving into “adult life.” They are interviewing for jobs, thinking about relocation, finding an apartment or a home, buying a car, making new friends and professional colleagues, and figuring out student loan pay-off schedules. It’s a really stressful time for most people entering the workforce now, and it warrants some extra attention.
The whole topic of onboarding has become more important in recent years. Competition for highly skilled employees is great and the cost of orienting a new employee is large and takes months in some cases. Hiring the right employee, welcoming and training them well, and then keeping them for a long time is the most cost effective path. First year turnover rates are high in the healthcare industry, which is, paradoxically, an industry that is full of compassionate and caring individuals, but also with a strong history of “eating their young” – the practice of challenging new staff in an exaggerated way to see if they are strong enough to stand up to the demands of the job over time.
I’d like to talk about what successful onboarding looks like. A newly graduated professional is a little bit of a unique situation. In some respects, they want the same things as new employees as anyone: to be welcomed and treated with respect, a pleasant workplace, and work that is both manageable and intellectually stimulating. A new grad, though, is also learning a lot of practical applications of the knowledge they acquired in the academic setting and maybe unlearning a few things that worked in academia but aren’t applicable in the “real world” of their new job. They are still figuring out the new reality of what things they own as a professional and what things they need permission for as an employee. It’s hard. If we want to encourage strong retention, we can’t ignore all the changes the new grad is experiencing over and above the already stressful transition of starting a new job. It is imperative that we help these new pharmacists find a work/life balance, support their needs for learning as well as camaraderie, and keep in close contact with them for that first year on the job.
So what can we do as leaders to support successful onboarding? I think the first thing that needs to happen is that we have a good onboarding plan. It is helpful to have a checklist of activities that need to happen around starting a new employee – and you need to actually use it. The kinds of things that are typically on such a checklist are:
· Make a post-acceptance follow-up call to cover things like where to park on the first day, what time to report for duty, dress code, etc.
• Complete necessary IT and Telecom requests to have as much as possible ready to go prior to the start date.
• Order business cards, office supplies, etc., as applicable.
• Communicate to the rest of the staff to announce the new hire and planned start date. Post a picture if possible.
• Schedule mandatory orientation and other training classes.
• Share the department work schedule.
• Conduct department/building tours – include places like the cafeteria, the library, commonly used meeting/training rooms.
Carle’s onboarding checklist actually maps out activities for the first full year of employment.
I think the second thing that we can do – and this is especially true for a new grad – is pair them right away with an “onboarding partner” or “mentor.” Having someone with some tenure in the department assigned as a mentor encourages an immediate personal connection with at least one other person and with the department as a whole. Our mentors schedule regular meetings with their mentees. They have some meals together. They talk about how training is going. The mentors field a lot of questions about almost everything and are able to re-direct the new employee to the best source of information for the questions they can’t answer. The mentor group also meets together to talk about the mentoring program and continually look for ways to improve.
I think the third important support that can be provided is for the department leader to take an interest in the professional development of the new grad. At its simplest, this might just mean frequent meetings to touch base and determine how training is going and whether the new grad has any concerns or questions. We require a minimum of a 1-week, 30-day, 90-day, and 1-year check-in, but in reality, we meet much more frequently than that to orient a new grad pharmacist.
We start those development conversations right away with all new pharmacists, but it is especially important for new grads, who may not have given much thought to ongoing training and development needs. I think it is important and relevant for the new grad to understand that attaining the degree doesn’t translate to being finished with learning. The goal of the initial meetings is to ascertain the new grad’s interests and devise a development plan that will capitalize on those interests and allow for professional development and movement into increasingly complex roles within the organization. And in fact, the early goals might be continued career exploration to help the new grad crystalize their thoughts on what those interests really are. Ongoing meetings must be scheduled to track progress with the plan. Within the first year, we are starting to have the conversation about exploring board certification, either as a generalist or selecting an area of focus such as nutrition or oncology. We then work toward preparation for the exam such that by the time they meet the other qualifications for certification, they are ready to test.
Onboarding new grad pharmacists represents a special challenge in helping the fledgling professional to learn to fly on their own. I hope this has given you some ideas on how to successfully approach this important transition.
 Directly Speaking
Directly Speaking
The ENE Society: How Fun and Networking Can Go Hand in Hand
by Scott A. Meyers, Executive Vice President
In 1998, I became a member of a semi-secret society called the ENE Society. Semi-secret, in that we don’t tell people about why it’s called the ENE Society, how it came to be and most importantly what happens when we meet. But not to fear, it’s pretty much a dining and networking group that meets twice a year at the ASHP Summer and Midyear Clinical Meetings, wherever they may be held. Oh, and also at the Texas Society of Health-System Pharmacists Annual Seminar (their version of our Annual Meeting, or vice versa).
In fact, the Society was founded in Texas in response to some exclusionary behavior of a few key national dignitaries. It was originally formed in jest but with the sincere mission of being inclusionary rather than the former. The three initial or founding ENEs, as we are called, slowly expanded their circle to a group that now includes a membership that is nationwide! I was fortunate to be one of the first (but not the original) non-Texan to be inducted into the Society and have missed only one dinner since the Midyear of 1998, and only because a temperature of 103° had me in a Las Vegas hospital emergency room.
With that brief, albeit as complete as I possibly can make it without getting drummed out of the Society, explanation of what the ENE Society is and does, I want to share why it has become so important to me. The ENE Society is networking at its highest level for me, not to say if Bill Gates called and asked me to begin networking with him and his buds that I might withdraw or reclassify that statement a bit. But that’s not going to happen, and even if it did, the genuineness and value of the relationships I have formed with my fellow ENEs are priceless and ones I wouldn’t trade. And here’s why:
They are Practice Leaders – Many, if not most, of this group are practice leaders in pharmacy. I say most because I certainly am not but work hard to support our practice leaders and all practitioners in Illinois. These ENEs are Pharmacy Directors, Chief Pharmacy Officers, Clinical Specialists and association volunteer leaders. They provide me with another perspective on practice that I don’t see every day from my desk. They are practice leaders just like each of you are or can be!
They are Practice Leaders from around the Nation – The members of the ENE Society come from all over the US. I don’t believe we have any international members yet, but the day could be fast approaching. Many of these individuals have been presidents of their respective State Society of Health-System Pharmacists, and at least half a dozen of them have served as ASHP’s top elected leader! They can provide me with input and perspectives at the association level, too. Illinois needs more nationally recognized practice leaders, so here’s your next step should you choose to take it.
They are Givers – These individuals give more than they receive. They try to help others even with no chance of payback in the picture. They are connectors and helpers. They will help you solve a problem, and if they can’t, they will try to connect you with someone who they think can. While some people who have climbed leadership ladders within pharmacy associations are takers, you won’t find any in this group. I’m pretty sure that’s a mandatory criterion for induction into this esteemed assembly. I know lots of givers within ICHP, and if you’re not sure you are, that’s something you can easily work at.
They are Fun – Almost as important a criterion as being a giver, these folks like to have fun. Yes, the initial induction includes a very limited and good natured hazing, but after that is done, it’s one for all and all for fun. Because pharmacy, like most professions, generates a significant amount of day-to-day stress, the group loves to let loose when they are together. I often have the privilege or responsibility of identifying a restaurant for our semi-annual ASHP gatherings, and the first question I ask the restaurant staff when making a reservation, is whether they have a private dining room or someplace in a corner, because this group is kind of loud. Each member of the group enjoys the others’ company, and yes, we do get a little loud from time to time. But with dynamic leaders come dynamic personalities. Oh, and I know we have some fun personalities within ICHP! And we can always use more. We need to break the stereotype of the quiet and boring pharmacist for good!
A handful of ENEs reside in Illinois these days. And I’m sure in the future there will be more Illinois ENEs unless some zombie apocalypse or global disaster halts domestic travel for a significant amount of time. While I’m not a practice leader, I appreciate the connection I have with those who are, and I know they appreciate me for who I am and what I do. We are colleagues, friends and association champions. We carry pharmacy’s banner wherever we go, together or apart, and we talk to each other frequently throughout the year to solve some of pharmacy’s many problems. You’d be surprised what you can accomplish when you know the people you need, when you need to get a job done.
I’m fortunate to be an ENE, but each of you can form your own semi-secret society of friends and colleagues to make each other’s lives better and fuller. And if you want to induct me into your semi-secret society, I will do my best to make it work for you!
New Practitioners Network
More than a 9 To 5 Pharmacist: Adding Value to the Team
by Heather Malcom, PharmD, PGY1 Pharmacy Resident HSHS St. John’s Hospital
In recent years, a paradigm shift has occurred within pharmacy. Prior to the shift, the focus was on avoiding patient harm. Today the focus is on improving patient care. As new practitioners, our pharmacy school curriculum provided clinical education and training allowing us to be confident as clinical pharmacists on interdisciplinary teams. As the pharmacy practice model continues to shift towards a clinical focus, it is essential that we become value-added team members and help advance the pharmacy department instead of relying on management alone. This can be done through the following three methods.
Ensure strong clinical skills
Strong clinical skills are imperative to improve the pharmacy department’s clinical services. Ways to improve clinical skills are by providing department in-services and reviewing medication error reports to identify areas for improvement. Other ways to ensure strong clinical skills include encouraging professional organization memberships and providing continuing education presentations during the lunch hour. Becoming an ICHP site champion is a great way to encourage organization involvement from the whole department and provide continuing education to enhance clinical skills.
Identifying needs of the team
As pharmacists move out of the pharmacy and onto patient care floors, we should look for ways to improve patient care. Identifying the most common chronic disease states of the population, frequent medication errors, and medication specific Centers for Medicare & Medicaid Services (CMS) quality measures are starting points. Once areas for improvement are identified, pharmacists should initiate the development of policy and protocol changes. This may include patient discharge counseling for chronic disease states with high readmission rates, education to prevent frequent medication errors, or medication usage evaluations for frequently misused medications.
Committee involvement
A strong pharmacy presence within the hospital can promote the department’s clinical services and improve pharmacy processes and policies. As value-added team members, we can help management by representing pharmacy at different hospital department meetings. The benefits of committee involvement are far-reaching. Increasing the pharmacy department’s presence can lead to new clinical services. At my institution, areas for improvement were identified within the medication reconciliation process; as a result, pharmacists will work in collaboration with hospitalists to ensure a smoother transition of care at discharge. Another benefit of committee involvement is building strong relationships with other departments. Direct communication helps identify areas for process improvement and will hold each department accountable.
As new practitioners, we can make impactful changes even if we are not in management positions. We can add value to the team by taking the initiative to ensure strong clinical skills of all pharmacists, advance clinical services provided by the pharmacy department, and become pharmacy representatives for different committees.
References
1. An era of growth and change: a closer look at pharmacy education and practice. (Feb 2014). http://www.ucop.edu/uc-health/_files/pharmacy-an-era-of-growth-and-change.pdf. (accessed 2015 May 23).
2. Jorgenson D, Dalton D, Barbara F, et al. Guidelines for pharmacists integrating into primary care teams. Can Pharm J. 2013; 146(6):343-352.
3. Tyrrell R. How to introduce pharmacists to the primary care team. (March 2015). http://www.advisory.com/research/care-transformation-center/care-transformation-center-blog/2015/03/integrated-pharmacy-models-in-primary-care. (accessed 2015 May 23).
Leadership Profile
by Matt Nelson, BS, PharmD, BCPS
 What is your current leadership position in ICHP?
What is your current leadership position in ICHP? Co-advisor for the Roosevelt University College of Pharmacy SSHP Chapter
Where did you go to pharmacy school?
University of Illinois at Chicago
Trace your professional history since graduation: where have you trained / worked, any special accomplishments?
PGY1 Residency of University of Chicago. PGY2 residency in Internal Medicine at University of Chicago- I was chief pharmacy resident during my PGY2 year. After finishing residency, I took a position as an assistant professor at Roosevelt University College of Pharmacy. I currently coordinate courses covering gastrointestinal and liver therapeutics, special patient populations, and specialty pharmacy, as well as serving as chair of the admissions committee.
Describe your current area of practice and practice setting
My practice site is at Rush University Hospital working with their inpatient general medicine services. We serve a very diverse and complex patient population, so every day gives me an opportunity to learn about something new.
What initially motivated you to get involved, and what benefits do you see in being active in a professional association such as ICHP?
ICHP provides a network for new practitioners who want to be involved in the development of pharmacy practice locally and throughout the state. I initially became involved with the student chapter because we have a very active group of students interested in maximizing their experience preparing for their future careers and training. I enjoy providing them with guidance as they pursue this goal.
Is there an individual you admire or look up to, or a mentor that has influenced your career?
I have had a lot of mentorship over the last few years, both as a student and a resident. Every time I discuss chronic kidney disease with students on my rotation, I still try and emulate the approach that my PGY2 director, Leah Bentley, showed me when I was a resident on her service. I also learned a lot about patient and practice management from Ishaq Lat at University of Chicago. I feel like I could list all of my preceptors from residency for this question, as each of them has affected either my practice or teaching methods in some way.
Do you have any special interests or hobbies outside of work?
I really enjoy cooking. If I wasn’t a pharmacist, I would want to go culinary school. I am also a huge fan of the Chicago Blackhawks.
Do you have a favorite restaurant or food?
The ceviche at Frontera Grill is amazing; it’s one of my very favorite things.
What is your favorite place to vacation?
My wife and I took a really spectacular trip to Italy last year. If I could go there every year I would.
What is the most interesting/unique fact about yourself that few people know?
I am a dual citizen of the U.S. and Canada. My parents are from Wisconsin, but moved to Ontario, where I was born, and they didn’t move back to the States until I was 6 years old.
What 3 adjectives would people use to best describe you?
Patient
Fun
Team-player
Government Affairs
Statutes and Regulations Move in April!
by Jim Owen and Scott Meyers
April was a crazy month and seemed to fly by as far as legislation and regulation go. The Illinois Departments of Financial and Professional Regulation and Human Services were able to promulgate new rules for the Controlled Substance Act and the Pharmacy Practice Act. These rule changes have been in the pipeline for a long time, and ICHP has provided input all along the way. Rather than provide you with a detailed list of the changes the entire rules changes can be found on the ICHP Website www.ichpnet.org on the Public Policy page by clicking on the “
Pharmacy Practice Act and Other Related State Statutes” link.
We have provided some highlights of the changes:
Highlights of the Illinois Pharmacy Practice Act Rules revisions
1. Unprofessional and Unethical Conduct 1330.30 –
a. Failing to exercise sound professional judgment with respect to the accuracy and authenticity of any prescription/drug order dispensed.
b. Committing dispensing error that results in hospitalization of a patient or demonstrating a pattern and practice of dispensing errors.
c. Willfully violating or knowingly assisting in the violation of any law relating to the use of habit forming controlled substances.
2. Violations 1330.40 – If a licensee or registrant is disciplined in another state, he or she must inform the Division (Professional Regulation) within 60 days.
3. Renewals 1330.80 – Pharmacy technicians shall be required to submit with their second renewal, proof of certification as a certified pharmacy technician, proof of enrollment in a first professional degree program in pharmacy or proof of enrollment in a clinical training program by a graduate of a foreign pharmacy program.
4. Application for Certificate of Registration as a Pharmacy Technician 1330.200 –
a. No person with an active Illinois pharmacist license may hold an active Illinois pharmacy technician registration.
b. Any student pharmacist who is expelled or drops out of a first degree program in pharmacy, fails to complete their 1200 clinical training within 24 months or fails the pharmacist licensure examination three times must notify the Department within 10 days and must become registered as a certified pharmacy technician within 90 days.
5. Pharmacy Technician Training 1330.210 – Responsibility for training of pharmacy technicians and certified pharmacy technicians is now jointly shared by the pharmacy, the Pharmacist in Charge and the pharmacy technician.
6. Application for a Pharmacy License 1330.400 –
a. Any reduction of hours of operation shall be reported to the Division within 30-days.
b. No pharmacy shall relocate prior to the inspection of the premises. All drugs shall be transferred within 24 hours after issuance of the license unless otherwise approved by the Department.
7. Community Pharmacy Services 1330.500 –
a. Any drugs dispensed pursuant to a prescription, other than vaccinations administered in the pharmacy, shall have affixed to its container a label as provided in the Act.
b. Any mail order pharmacy that provides services in Illinois shall provide, during its regular hours of operation, but not less than 6 days per week for a minimum of 40 hours per week, a toll-free telephone service to facilitate communication between patients and a pharmacist retained by the mail order pharmacy. The toll free number must be included on the prescription label.
8. Telepharmacy 1330.510 – There are a substantial number of clarifications provided in this section. Anyone considering the use of or currently using telepharmacy services should review this section in depth.
9. Onsite Institutional Pharmacy Services 1330.530 –
a. Medications dispensed to patients at discharge must now contain directions for use on the label.
b. An automated dispensing and storage system may be used as an afterhours cabinet.
10. Security Requirements 1330.600 – Removes the restrictions for handling and storage of CII medications in the pharmacy and when the pharmacist is not present.
11. Pharmacy Structural/Equipment Standards 1330.610 – All pharmacy dispensing and drug storage areas must be contiguous except for on-site institutional pharmacies.
12. Pharmacist in Charge 1330.660 – If a pharmacist in charge is on a leave of more than 90 days, a new pharmacist in charge must be designated.
13. Automated Dispensing and Storage System 1330.680 – Any medication error resulting from the use of an automated dispensing and storage system that results in a patient hospitalization (new) or death must be reported to the Department within 30 days after acquiring knowledge of the incident.
14. Reporting Theft or Loss of Controlled Substances 1330.710 – The Department now requires that when filing the DEA Form 106, a copy is be sent to the Department concurrently Attention of Drug Compliance Unit.
15. Multi-Med Dispensing Standards for Community Pharmacies 1330.740 – Multi-Med Paks that have been delivered to an institution, patient or patient’s agent may be accepted for return to the pharmacy only when a medication must be added or removed or when drug therapy is discontinued. Med-Paks returned to the pharmacy may only be re-dispensed for the same patient. The revised med pak shall be given a new serial number.
16. Return of Drugs 1330.750 – The prohibition of return of medications to a pharmacy once they have left the premises does not apply to medications returned as a result of medication error or drug recall. These medications may not be reused.
17. Pharmacy Self-Inspection 1330.800 – This is a new section. All pharmacies are now required to conduct annual self-inspections and retain completed self-inspection forms for 5 years.
Highlights of the Illinois Controlled Substance Act Rules revisions
1. Schedule II, III, IV, and V Drug Prescription Requirements 2080.70 –
a. A prescription for a Schedule II, III, IV, or V drug shall have affixed to the face of the prescription the prescriber’s electronic or handwritten signature, initials, thumbprint, or other biometric or electronic identification process approved by IDFPR.
b. A prescription for a Schedule II medication shall not allow more than a 30-day supply on any one prescription.
c. A prescription for a Schedule II medication shall not be refillable (this is new in the rules, believe it or not)
d. A prescriber may write three sequential prescriptions for a 30-day supply of a Schedule II medication.
2. Dispenser Responsibility 2080.100 – Reports submitted to the PMP by the dispensers of controlled substances must now include the new fields:
a. Dispenser full name and address
b. Prescriber full name
c. Date dispensed
d. Payment type
e. Patient location code (home, nursing home, outpatient)
3. Reports 2080.190 –
a. This section now allows prescribers, dispensers or patients to request reports of usage.
b. It also allows the Department of Human Services staff to generate reports to prescribers and dispensers when doctor shoppers or pharmacy shoppers are identified by 6 or more purchases in a 30 day period.
c. This section creates operational report capability for the Department including trend analysis.
d. Aggregate data from the PMP may be used for clinical studies.
4. Access to the Prescription Information Library (PIL) 2080.210 – Allows for the creation of group user for pharmacies, emergency rooms or physician offices.
5. Error Reporting 2080.220 – A new section that allows prescribers and dispensers to report errors in their PMP prescribing or dispensing information.
6. Designated Controlled Substances 2080.230 – Now allows the Department on the recommendation of the PMPAC (Prescription Monitoring Program Advisory Committee) to designate drugs into Scheduled Controlled classes.
7. Mid-Level Practitioners Prescriptive Authority Reporting 2080.240 – This section requires physicians who delegate prescriptive authority to Mid-Level Practitioners must enter the prescriptive authority delegation into the PMP including controlled substances delegated to prescribe.
8. Mailing of Controlled Substances 2080.250 – Controlled substances are now allowed to be mailed within the U.S. and this section describes the requirements for the mailing containers. Controlled substances may not be mailed internationally.
9. Definitions 3100.10 – "Pre-printed Prescription" means a written prescription upon which the designated drug has been indicated prior to the time of issuance, including any pre-inked stamp that would be applied to a prescription blank. The term does not mean a written prescription that is individually generated by machine or computer in the prescriber's place of business.
10. Exemption of Agents and Employees 3100.80 – In a licensed hospital, hospital affiliate, or licensed ambulatory surgical treatment center ("institution") a licensed advanced practice nurse, acting pursuant to Section 65-45 of the Nurse Practice Act, or a physician assistant, acting pursuant to Section 7.7 of the Physician Assistant Practice Act of 1987, may be granted clinical privileges, including the authority to select, order and administer, and issue discharge prescriptions for, controlled substances under the DEA registration number of the hospital, hospital affiliate or licensed ambulatory surgical treatment center by whom he or she is employed. Mid-Level practitioners must be credentialed by the hospital medical staff to select, order, and administer and issue discharge prescriptions for controlled substances.
11. Security Requirements Generally 3100.310 –
a. Personal bags including purses, handbags, and backpacks are prohibited in any area where controlled substances are handled or stored.
b. A basic alarm system that detects unauthorized entry into the pharmacy is required of pharmacies not open 24-hours a day.
12. Physical Security Controls for Practitioners 3100.340 - All Schedule II controlled substances shall be stored in a securely locked, substantially constructed cabinet.
13. Record and Inventory Requirements Generally 3100-360 –
a. Every licensee shall conduct an annual inventory that includes an inventory with an actual count of the inventory on hand for all Schedule II controlled substances and an approximate inventory for all Schedule III, IV, and V controlled substances. The inventory shall be maintained for a period of not less than 5 years.
b. After a loss or theft of controlled substances, a licensee shall conduct an approximate count inventory with a start date of the last inventory for the controlled substance that was either lost or stolen.
14. Requirements of Prescriptions for Schedule II Controlled Substances 3100.400 –
a. A pharmacist may not change the following components of a prescription for a Schedule II controlled substance:
i. Date written, or add a date
ii. Name of the patient
iii.Name of the prescriber, or add a prescriber, and
iv.Name of the drug
b. Any other components of a prescription for a Schedule II controlled substance may be changed after consultation with the prescriber.
These are just the highlights of the changes made to the Illinois Pharmacy Practice Act Rules and the Illinois Controlled Substance Act Rules. It is the responsibility of every licensed pharmacist, registered pharmacy technician and student pharmacist to review and become familiar with these changes.
And if that wasn’t enough, the General Assembly is in full swing, in fact, getting closer to the normal end of session and crunch time, and we’ve been incredibly busy working with legislators and others on several key pharmacy bills. First and foremost this session is House Bill 1 or HB1. We have worked with the Illinois Retail Merchants Association (IRMA) and the Illinois Pharmacists Association (IPhA) to address the several significant and undesirable sections of the first House amendment to HB1 and have succeeded in removing all of pharmacy’s biggest concerns. The mandated pharmacy hosted medication take-back programs have been stripped from the bill as has the 10-day Schedule II supply limit. In addition, the pharmacy associations have worked with the Medical Society and a large coalition of most all of the health related professions to address a variety of other issues regarding screening, reporting and access to opioid antagonists. At this time ICHP is now a proponent of HB1 as amended with House amendment 3.
The biosimilar interchangeability issue remains hot. The proponents of SB1611 sponsored by Senator Tony Munoz, have continued to push for mandatory reporting of interchange of an FDA approved interchangeable biosimilar even though the FDA themselves do not have that requirement and states “An interchangeable product may be substituted for the reference product without the intervention of the health care provider who prescribed the reference product.” ICHP is continues to work with our pharmacy allies and the proponents to obtain an exemption to this reporting for all hospitals and health-systems and their wholly owned infusion centers and physician clinics.
HB3271 that would require continuing pharmacy education for certified pharmacy technicians has been held up by the sponsor, Rep. Mike Zalewski as a means of forcing pharmacy to support a separate bill requiring the use of locking medication vials for all Schedule II controlled substances. Pharmacy is working toward a compromise with Rep. Zalewski that would create voluntary or grant-funded pilot projects for the use of the medication locking vials but because of the vials’ cost (current retail cost is over $15 each), pharmacy cannot support any mandate of their use without subsequent reimbursement.
HB3627, the expanded pharmacist immunization bill, hit a brick wall with the pediatricians and as a result of that the Illinois State Medical Society. A new revised bill HB4213 has been introduced that would expand pharmacist administration of meningitis and MMR vaccines to patients age 10-13. The bill would require the usual reporting but would also add a mandatory pharmacy reporting to the Illinois Comprehensive Automated Immunization Registry of all immunizations administered to patients under the age of 18. Currently, there is limited hope that this bill will move during this session.
March, April and May are usually the busiest months of changes in Illinois statutes and regulations, and this year looks to be a record-setter! The ICHP Division of Government Affairs is working on these and a few additional issues every month, and we encourage you to be more informed and active in the efforts on behalf of pharmacy’s future.
Professional Affairs
Improving Tdap Vaccination Rates among Infant Caregivers
by Zachary Pentoney, PharmD; Despina Kotis, PharmD, FASHP
Introduction
The advent of vaccines ushered in a new era for public health. When the pertussis vaccine was introduced in the 1940s, the case rate of pertussis was roughly 150,000 cases per year. By the 1980s, the case rate had fallen to less than 10,000 per year. Since the 1980s, the number of reported cases of pertussis has slowly increased, with 28,660 cases reported for 2014.1 Of note, the incidence of pertussis is highest for infants younger than 12 months of age, and infants 2 months of age or younger are particularly vulnerable as they are ineligible for vaccination due to young age. In fact, 7 of the 9 pertussis-related deaths in 2014 were infants less than 3 months of age.2
In 2011, the Advisory Committee on Immunization Practices (ACIP) recommended that mothers and close contacts of neonates (e.g. siblings, grandparents, etc.) be vaccinated with Tdap (tetanus toxoid, reduced diphtheria toxoid and acellular pertussis) vaccine to protect neonates. This strategy is called “cocooning” as the process of vaccinating the infant’s closest contacts creates a protective cocoon around the infant, helping to insulate him or her from pertussis. Sadly, cocooning initiatives have had mixed results. According to unpublished data from the CDC, these programs have been most successful among post-partum mothers, but there is still room for growth in reaching other family members like fathers.3
Process
In November 2013, Northwestern Memorial Hospital (NMH) implemented a caregiver Tdap vaccine initiative to improve caregiver access. NMH is an 894-bed academic medical center with 12,497 live births for fiscal year 2014. The initiative was targeted at parents and other caregivers expected to have close contact with the neonate. The process is as follows: 1) caregivers present to Northwestern to visit the neonate; 2) nursing staff identify which caregivers have “close contact” with the neonate and provide education regarding the importance of the vaccine; 3) willing caregivers sign a consent form; 4) nursing staff administer the vaccine and document administration in the neonate’s electronic health record (EHR); 5) pharmacy staff document caregiver receipt in the Illinois Department of Health Immunization Registry (I-CARE) database. The program is currently funded with grant money donated by the Northwestern Medical Faculty Foundation and covers the cost of the vaccine.
As noted in Figure 1, there was considerable fluctuation in the number of doses dispensed from November 2013 to April 2015. The average number of doses dispensed during this time frame was approximately 70 per month. It is important to note that these figures represent electronic records of doses dispensed, not actual doses administered. Figure 2 shows the number of doses administered based on relationship to the infant for the time period August 2014 to March 2015. Of note, a majority of the doses administered were to fathers. Grandparents were the second most common relative to be vaccinated in the post-partum period. From August 2014 to April 2015, the vaccination rate among fathers declined and then leveled off at about 50% of the August 2014 rate.
Lessons Learned
A hospital-based cocooning program requires a multidisciplinary approach to be successful. Physicians agree to provide a standing order so that nurses and pharmacists can evaluate patient vaccine eligibility and administer the vaccine. As those on the front lines, nurses serve as the initial resource for answering caregiver questions about the vaccine. Additionally, nurses administer the vaccine and perform preliminary documentation. All of this is incorporated into nursing workflow. Furthermore, the pharmacy department agrees to provide the vaccines and finalize the documentation. An initial challenge for the program was workflow adjustments during busy periods.
The apparent decline in vaccination rate of fathers between August 2014 and April 2015 could be due to a variety of factors. Some nurses at Northwestern have speculated that fathers may be getting vaccinated elsewhere (e.g., community pharmacies) prior to coming to the hospital. Additionally, some have suggested that seasonal variation in birthing rates (higher in the summer months compared to the winter months) may account for part of the variation seen. Although the program currently tracks which caregivers receive Tdap vaccine, there is no process in place to capture how many caregivers are not reached or have refused the vaccine. This would be valuable information as it could indicate how effective the program is in facilitating a “complete” cocoon (all caregivers with close contact vaccinated). Furthermore, this new data would provide insight into the apparent decline in vaccination rates and illuminate opportunities for improvement.
Another key aspect of the program is ensuring the safety of caregivers and health care professionals during the vaccine administration process. On one occasion, a nurse sustained a needle stick injury while administering the vaccine to a caregiver. Although the hospital had policies in place regarding vaccine safety and accidental needle sticks, there was no clear provision for how to handle a needle stick when a “non-patient” was involved. Consequently, new language was proposed for the caregiver consent form so that in the event of a needle stick accident, the hospital would be permitted to obtain blood samples from the caregiver to provide adequate care for the injured worker.
Future Initiatives
Moving forward, a revised consent form will be brought to Northwestern’s medication safety subcommittee. Additionally, a survey that could potentially help capture reasons why caregivers may decline the Tdap vaccine is being developed. Lastly, funding to sustain the program is being sought.
Conclusion
A hospital-based Tdap program aimed at vaccinating close contacts of neonates can successfully reach close relations like fathers who have previously been difficult to reach. The success of such a program hinges on collaboration between members of the health care team. Even if caregivers decline the vaccine, they are receiving education and may decide to get vaccinated later. By implementing an inpatient-based Tdap program, institutions can give back to the community and contribute to public health.
Figure 1. Total number of post-partum Tdap doses dispensed from automated dispensing cabinets (ADCs).
Figure 2. Total number of post-partum Tdap doses administered to caregivers over time based on caregiver relationship to the neonate. Data are taken from paper copies of vaccine administration paperwork. Other category includes: nanny, great grandparent, godparent, grandnephew, and not otherwise specified.
References
1. Centers for Disease Control and Prevention. Pertussis (Whooping Cough): Surveillance & Reporting. Updated 2014 Jan 2. Accessed 2015 Apr 16. Available at: www.cdc.gov.
2. Centers for Disease Control and Prevention. National Center for Immunization and Respiratory Diseases, Division of Bacterial Diseases. 2014 Provisional Pertussis Surveillance Report. January 9, 2015.
3. Centers for Disease Control and Prevention. Updated recommendations for use of tetanus toxoid, reduced diphtheria toxoid and acellular pertussis vaccine (Tdap) in pregnant women and persons who have or anticipate having close contact with an infant aged <12 months – Advisory Committee on Immunization Practices (ACIP), 2011. Morbidity and Mortality Weekly Report. 2011;60(41):1424-1426.
4. Red Book Online [database online]. Greenwood Village, CO: Truven Health Analytics, Inc. Updated periodically. Accessed May 13, 2015.
Educational Affairs
Tricyclic Antidepressant Related Adverse Effects Based on Neurotransmitter Modulation: Selection for Adjuvant Analgesia
by James Blazier, PharmD; Lindsey Reno, PharmD; Chris Herndon, PharmD, FASHP
Introduction
Tricyclic antidepressants (TCAs) have been used clinically for various indications for over 50 years. Imipramine, the first TCA, was developed as a phenothiazine derivative for the treatment of major depressive disorder. These drugs work by blocking the removal of serotonin and norepinephrine from the synapse which in turn increases the levels of the neurotransmitters available for binding with receptors.1 These drugs also block the a1, H1, 5-HT2, and muscarinic receptors. Amoxapine additionally has some activity as a nonselective dopamine receptor antagonist.2
TCAs have been utilized for many years to treat depression although their use for this diagnosis has largely fallen out of favor as first or second line options due to their side effect profile at required doses. Despite this, these drugs have still found a significant role in the treatment of neuropathic pain, insomnia, resistant depression, and the prevention of migraines.2,3
Frequently these drugs are chosen based on their side effect profile. Side effects for this class of agents vary between agents. Predicting severity of individual side effects of TCAs is difficult, which can make selection of the best patient-specific treatment difficult. Examination of TCAs binding affinity constants (Ki) may assist the clinician in predicting side effect burden. The binding affinity constant is the concentration of index drug needed to decrease the rate of the reaction by half. The smaller the Ki the smaller the amount of the drug is needed to inhibit the activity of the enzyme.4 For instance, doxepin has a Ki 0.24 nM compared to desipramine which has a reported Ki of 110 nM for the histamine receptor. Thus, doxepin is approximately 300 times more potent in its antihistamine activity.
Previous, binding affinities for various neurotransmitter receptors or transporters was associated with theoretical differences in both efficacy and side effect profiles of neuropharmacologic agents. Recently, reported incidence of these side effects and correlated receptor or transporter binding affinities have been reported.5
Serotonin
Serotonin reuptake inhibition is associated with various side effects depending on which receptor subtype is being inhibited. Inhibiting 5-HT is associated with nausea, diarrhea and sweating. Inhibiting the reuptake 5-HT1A is correlated to dizziness, 5-HT1A insomnia, 5-HT2A dizziness, insomnia, sedation, sleepiness, and weight gain, 5-HT2C dizziness, sleepiness and weight gain, 5-HT3 weight gain, and 5-HT7 insomnia and sedation.5 Based on Ki values presented in Table 1, clomipramine has the propensity to exert more serotonergic side effects, while doxepin on the other hand may exert the least. What this translates to clinically is that the incidence of dizziness, insomnia, sedation, and weight gain may be more prevalent in clomipramine than doxepin.
Pain relief associated with serotonin may be explained by its peripheral actions. In the peripheral nervous system serotonin invokes different actions than in the central nervous system (CNS). Here, serotonin serves as an inflammatory mediator as it is released from platelets and mast cells following tissue injury. Serotonin receptor subtypes have also been detected in dorsal root ganglia which suggests that these receptors are present on peripheral sensory nerves. The release of serotonin into inflamed or injured tissue can contribute to peripheral sensitization and resulting hyperalgesia.6
Norepinephrine
Inhibition of norepinephrine reuptake is associated with increased sweating, headache, increased heart rate, urinary retention, and anxiety/restlessness.3,5 Based on reported Ki values, desipramine would have the greatest affinity at the norepinephrine transporter receptor and clomipramine would have the least. The greater the affinity for blockade of the norepinephrine receptor, as described in Table 2, the greater the prevalence of the aforementioned symptoms due to increased norepinephrine synaptic concentration.
Along with serotonin, norepinephrine is involved in pain modulation via the descending inhibitory pathway. Some pain syndromes, such as fibromyalgia, are associated with a deficient endogenous inhibitory pain system.7 These defects in this inhibitory pathway could be explained by an imbalance of norepinephrine and serotonin concentration levels.7 Interestingly, clinical studies in chronic pain syndromes have been largely disappointing with either selective serotonin or selective norepinephrine reuptake inhibitors, yet nonselective reuptake inhibition appears to yield antinociceptive activity.
Muscarinic
Antagonism of the muscarinic receptor is associated with anticholinergic side effects. Some of these side effects include dry mouth, urinary retention, increased heart rate, drowsiness, and confusion. It is important to note other possible medications a patient may be on when initiating a tricyclic to see if anticholinergic side effects would be enhanced. This is especially true in elderly patients. These patients have a higher propensity to experience these anticholinergic side effects, especially the confusion. If the muscarinic blockade is severe, these patients could develop delirium. For this reason, these high affinity muscarinic TCAs (amitriptyline), as described by the Ki values in Table 3, are not recommended in the elderly population.8
Alpha-1
Antagonism of the a-1 receptor is associated with hypotension, dizziness, insomnia, sedation, sleepiness, and weight gain.5 Based on the data provided in Table 4, trimipramine has the greatest affinity at the a-1 receptor and protriptyline has the least affinity. Thus, trimipramine has a greater chance of causing hypotension, insomnia, sedation, and weight gain than protriptyline.
Histamine
Antagonism of histamine is associated with sedation, daytime sleepiness, and weight gain.5 Looking at the Ki values in Table 5, doxepin has a higher prevalence of causing sedation and weight gain than desipramine. This is consistent with clinical experience. Doxepin, nortriptyline, and amitriptyline can be used as adjuncts for pain in patients with concurrent problems initiating or maintaining sleep.
Trials have been completed on histamine H1 knockout mice to examine histamine’s role in pain. Pain thresholds of knockout mice were compared with heterozygote and wild type mice using a series of tests (hot-plate, tail flick, tail pressure, paw withdrawal). The knockout mice showed an increase latency in response with these tests indicating that histamine plays a role in pain perception.9
Dopamine
Antagonism of dopamine reuptake is associated with hypotension, dizziness, insomnia, sedation, sleepiness, and weight gain.5 Based on Ki values as described in Table 6, nortriptyline will have a greater incidence of dizziness and insomnia while doxepin will have little incidence.
Dopamine transporter metabolism defects may lead to increased pain. Neurodegenerative diseases that affect the dopaminergic system are associated with clinical pain symptoms. Dopamine agonists have been shown to relieve pain in these types of disease, as well as widespread pain syndromes (i.e. Fibromyalgia). Theoretically, TCAs that have the highest propensity for inhibition of dopamine reuptake, such as nortriptyline, may have a favorable outcome of decreased pain symptoms.10
Discussion
Using Ki values and associated adverse reactions can help guide TCA selection in certain clinical situations. For patients experiencing insomnia, doxepin would be a logical first choice due to the sedation associated with its affinity for the antagonizing the histamine and a-1 receptors but might have least effects on pain response due to the Ki of serotonin and norepinephrine. Assessing the Ki values for serotonin and norepinephrine reuptake inhibition may predict efficacy in pain management due to the association between serotonin, norepinephrine and analgesia. When discussing Figure 1, the combined Ki of serotonin and norepinephrine, desipramine, nortriptyline, and protriptyline may have the greatest effects on pain control. Nortriptyline could potentially be chosen by a clinician as an adjunct for pain control if increased sleep is a desired side effect. If sleep is not a desired side effect, desipramine may potentially be chosen as the adjunct TCA for pain.
Resources:
1. Lieberman J. History of the Use of Antidepressants in Primary Care. J Clin Psychiatry. 2003;5(7):6-10
2. O'Donnell J.M., Shelton R.C. (2011). Chapter 15. Drug Therapy of Depression and Anxiety Disorders. In Brunton L.L., Chabner B.A., Knollmann B.C. (Eds),Goodman & Gilman's The Pharmacological Basis of Therapeutics, 12e
3. Lexi-Comp, Inc. (Lexi-Drugs). Lexi-Comp, Inc.; January 27th, 2015
4. Pharmacology Weekly [internet] Pharmacology Weekly, Inc. c2008 [cited 26 Jan 2015] Available from: http://www.pharmacologyweekly.com/articles/inhibitory-constant-Ki-drug-interactions
5. Michl J, Scharinger C, Zauner M, Kasper S, Freissmuth M, Sitte HH, Ecker GF, Pezawas L. A multivariate approach linking reported side effects of clinical antidepressant and antipsychotic trials to in vitro binding affinities. Eur Neuropsychopharmacol. 2014 Sep;24(9):1463-74.
6. Sommer C. Serotonin in pain and analgesia: actions in the periphery. Mol Neurobiol. 2004;30(2):117-25.
7. Arnold LM. The Pathophysiology, Diagnosis, and Treatment of Fibromyalgia. Psychiatr Clin N Am. 2010; 33: 375-408
8. Mintzer J, Burns A. Anticholinergic side-effects of drugs in elderly people. J R Soc Med. 2000; 93: 457-
9. Mobarakeh JI, Sakurada S, Katsuyama S, Kutsuwa M, Kuramasu A, Lin ZY, Watanabe T, Hashimoto Y, Watanabe T, Yanai K. Role of histamine H(1) receptor in pain perception: a study of the receptor gene knockout mice. Eur J Pharmacol. 2000 Mar 10;391(1-2):81-9.
10. Hagelberg N, Jaaskelainen S, Martikainen I et al. Striatal dopamine D2 receptors in modulation of pain in humans: a review. European Journal of Pharmacology. 2004; 187-192.
Board of Pharmacy Update
Highlights from the May Meeting
by Scott A. Meyers, Executive Vice President
The March 12th Board of Pharmacy Meeting was held at the James R. Thompson Center at Randolph and LaSalle Streets in Chicago. These are the highlights of that meeting.
IDFPR Secretary – Bryan Schneider, new IDFPR Secretary attended the meeting and provided a welcome to the Board members and the audience. Mr. Schneider formerly served as Walgreens’ corporate counsel, so as a lawyer, he has a significant understanding of pharmacy practice. He expressed a strong commitment to efficiency, effectiveness and transparency within the Department during his tenure, and because of his previous experience on the other side, this may be more than the usual bureaucratic promises. He also informed the Board that the Department intends to re-establish the electronic newsletter of a few years ago to better communicate to the pharmacy profession. Mr. Schneider remained for the entire public portion of the meeting.
New Pharmacy Practice Act and Controlled Substance Act Rules – Department Assistant General Counsel, Daniel Kelber informed the Board of Pharmacy that the new Pharmacy Practice Act Rules had been approved by the Joint Committee on Administrative Rules in late April and are published in the May 8th Illinois Register. In addition, since the last Board of Pharmacy Meeting, the most recent draft of the Controlled Substance Rules had also been approved. Details of these changes can be found in the Government Affairs Report.
DSQA Meeting – The FDA held its third midwest regional meeting to discuss progress on the implementation of the federal Drug Security and Quality Act enacted three years ago in response to the NECC disaster. At this meeting, the FDA sought reporting from the states on their efforts to regulate compounding. It was stated that the FDA does not automatically inspect newly registered 503b Outsourcing Facilities. They encouraged the states to assist. Illinois will not license a newly registered outsourcing facility until the FDA has completed an inspection. The local FDA office is very collaborative, and the Department staff will continue to work with them to oversee these entities. The Act calls for a signing of a Memorandum of Understanding (MOU) that describes the State’s responsibilities between the federal government and the State. If the State does not sign the MOU, compounding pharmacies that are not registered as 503b entities may sell no more than 5% of their total annual sales to out of state customers. With a signed MOU, the 503a entities may sell up to 30% of their annual sales to out of state customers. It was also announced that the California Board of Pharmacy has implemented a program to inspect all out of state pharmacies annually at the expense of the nonresident pharmacy. The Department has no intention at this time to follow that model.
Remedial Course of Clinical Experience Outline – The Department staff, with help from the Board of Pharmacy members, will be developing an outline for pharmacies who wish to offer a 30-hour course of remedial clinical experience for individuals who have failed the NAPLEX three times. The outline will provide guidance for each section of NAPLEX, and the instructions will recommend that the preceptor focuses on the areas of the candidate’s weaknesses. A sample should be presented to the Board at the July meeting.
2016 NABP District IV Meeting – The 2016 event is scheduled to be co-hosted by the Illinois Board of Pharmacy and the University of Illinois at Chicago. At the March meeting of the Board of Pharmacy, Phil Burgess reported that Dean Bauman of UIC had contacted Board member Phil Burgess asking if the meeting could be held in Rockford in order to showcase the new Rockford Campus. The Board did not agree and felt the meeting should be held in the downtown Chicago area. Dean Bauman has now agreed to co-host the meeting in Chicago in 2016.
Legislative Update – The March legislative update was presented by Scott Meyers, ICHP Executive Vice President. There are a significant number of bills impacting pharmacy this legislative session, and a summary of those bills appear in this edition of KeePosted in the Government Affairs Report.
MPJE Item Writing – Several Board members wrote new test questions (items) for the Multi-State Jurisprudence Examination in March. The purpose was to fill gaps that currently exist in the item bank. The recently approved changes to the rules of the Controlled Substance Act and Pharmacy Practice Act were limitedly included. New test questions will be tested for several months to ensure that they are psychometrically sound and legally defensible before they may be included in the scored portion of the test, so candidates taking the MPJE for Illinois in the next six months or so should focus on the old Pharmacy Practice Act and Controlled Substance Act and respective rules.
Clinical Course of Instruction Reviews – Usually, as the last item of business in the public portion of the Board of Pharmacy meeting, the Board reviews applications for clinical courses of instruction (1200 hours of clinical training required for foreign pharmacy graduates prior to obtaining eligibility to sit for NAPLEX). At this meeting, the Board members discussed a recurring issue that prevents timely approval of these petitions. That is that many preceptors complete the description of the course work with no indication that Illinois pharmacy law will be a component of the instruction. This is a critical piece, and no description of this component will result in a denial and request for a revision of the course description.
Next Board of Pharmacy Meeting – The next meeting of the Illinois Board of Pharmacy will be held at 10:30 AM on Tuesday, July 14th at the James R. Thompson Center in Chicago. The profession is welcome to attend the open portion of this meeting.
College Connections
Pharmacists’ Evolving Role in Diabetes Management
by Amy McGlin, P2, ICHP-SSHP Vice President Rosalind Franklin University of Medicine & Science, College of Pharmacy
")
Diabetes mellitus is an increasingly prevalent disease in the United States and it is imperative that healthcare providers utilize appropriate therapies for its management. Pharmacists are key healthcare providers who can positively impact health outcomes and provide clinical expertise for managing patients with diabetes. Pharmacists serve as experts for safe and appropriate medication use, providing education to patients and other healthcare providers in order to optimize glucose control.
Management of chronic disease states by inter-professional teams, in which professions work towards the goal of providing patient-centered care, is continuing to be a focus of the constantly evolving healthcare system. As pharmacists and pharmacy students, we understand the need to educate and empower patients with diabetes mellitus. With numerous medications and various devices for medication administration, education is an extremely important part of diabetes management. In addition to blood glucose, blood pressure is an important part of managing this patient population’s overall health.
On April 18th, the ICHP-SSHP Chapter at Rosalind Franklin University of Medicine and Science - College of Pharmacy participated in the Diabetes EXPO at McCormick
")
Place in Chicago, which was hosted by the American Diabetes Association. Students performed blood pressure screenings throughout the day for meeting attendees. After measuring and providing patients with blood pressure readings, we provided blood pressure management information and education leaflets. Meeting with community members and helping to educate was incredibly rewarding for the participating students. Patients and family members were able to ask questions of students and faculty members; and at the end of the day, we had screened over 300 patients.
The Diabetes EXPO is a great example of how we can help educate our community and demonstrate the pharmacist’s role in healthcare. Our college’s ICHP-SSHP would like to thank the American Diabetes Association for giving Rosalind Franklin University of Medicine and Science the privilege to attend this event for the past three years in a row and to share our insights as part of the diabetes inter-professional health care team.
")
Philanthropic Opportunities
by Neha Kapur, P4, UIC Rockford Past President
Being involved in pharmacy organizations, such as ICHP, offers students the opportunity to partake in a variety of projects, services and events. Some of these opportunities include attending conferences, socials and educational meetings. By becoming actively engaged in these events, students grow in several ways, whether it is improving their performance as leaders, gaining networking skills or discovering something new. One type of opportunity in particular that I have thoroughly enjoyed has been the philanthropy events hosted by both the student chapter and state affiliates of ICHP.
As a part of the UIC ICHP Student Chapter, the Rockford campus was invited by Dr. Kristi Stice to participate in the “This One’s for the Girls” event at Kishwaukee Hospital back in February. “This One’s for the Girls” annually celebrates women and helps them to live healthier lives by offering screenings and educational services in addition to free giveaways. UIC participated in the event by teaming up with Kishwaukee Hospital’s pharmacy department to provide education on the importance of medication adherence and keeping an updated medication list. Additionally, we created a poster about osteoporosis and stroke prevention. The event was a huge success. Over two days of the three-day event, we were able to talk with hundreds of women and give them ASHP's “My Medication List” pamphlets. Most of the women were very responsive and many were caretakers and they said the list would be extremely helpful for a loved one. Attending this event was deeply rewarding as I was able to help provide valuable information to these women and see the significant impact the pharmacy department was able to make.
Another event that I was both proud to help plan and participate in was the Feed My Starving Children (FMSC) volunteer outing with the New Practitioners Network (NPN). At FMSC, volunteers work as a team to package specially designed food (Manna Packs) to reverse or prevent malnourishment in children throughout the world. When ICHP went to the facility in Schaumburg, we, along with other volunteers, were able to package 113 boxes for children in Madagascar. These boxes contained over 24,400 meals which fed about 67 children one meal per day for an entire year. It was astonishing to see how much we accomplished in just two hours. After the volunteer session, a few of us went to lunch at P.F. Chang’s to meet others in the NPN and ICHP student chapters. Overall, the FMSC event and lunch was an amazing experience. Not only was I able to donate my time to a worthy cause, but I was also able to meet some great people.
One of things I have learned from participating in these philanthropic events is how much of an impact just a few hours of my time can make, whether it is related to health care or not. Another aspect that I very much appreciate is how philanthropy helps build compassion in people, which is an essential component of becoming a great health care professional. As a pharmacist, showing compassion to your patients is a crucial part of building trust with them and as a result, improving their outcomes. I am privileged to have had the opportunity to join ICHP in these noteworthy causes. If you are ever in a position to do the same, with or without ICHP, I encourage you to do so. I can assure you that in return, you will gain just as much as you give.
Student-Faculty Networking Social
by Dalila Masic, PS-2, ICHP Social Chair - Midwestern University Chicago College of Pharmacy
Throughout pharmacy school, the phrase “pharmacy is a small world” has been repeatedly mentioned. Initially, it may bring about some skepticism since there are over 300,000 licensed pharmacists in the United States. However, students who have attended networking events have found out that a mutual connection may help shape their career path along the way. The most accessible pharmacists that a student has are faculty members. Unfortunately, they are typically only interacting with students during lectures, resulting in minimal opportunities to talk to them on a more personal level. In reality, many faculty members are pleased to talk to students and provide advice about career goals or pharmacy in general if given the opportunity.
The ICHP chapter at Midwestern University decided to break the gap and host the first Student-Faculty Networking Social. The goal of this event was to provide students the opportunity to learn more about specific pharmacy practice sites while networking and building connections with faculty members along the way.
After months of planning, the networking social was held on Friday, March 13th at Midwestern University. Twenty-five students and seven faculty members were in attendance. The faculty members practiced in areas including ambulatory care, oncology, acute care, and internal medicine. Overall, we received great feedback from both students and faculty regarding the benefits of the Student-Faculty Networking Social. Students enjoyed networking with faculty members and asking career-based questions, while faculty members enjoyed being able to provide advice and put a face to a student’s name. We hope to make this a tradition for years to come and grow the attendance of students and faculty members at this event every year.
More
Welcome New Members!

| Priyank Shah |
|
| Denise Kolanczyk |
Jennifer Phillips |
| Lisa Edmond |
|
| Kathleen Darger |
Carol Aldred |
| John Hubbe |
Elizabeth Jochum |
| Nicole Bernardo |
|
| Janet Tsouklis |
|
| Jennifer Frakes |
|
| Ian Wilson |
|
| Dorine Sobers |
Elizabeth Engebretson |
| Latavia Pennymon |
|
| Joana Ilijevski |
|
| Natalia Grushchak |
|
| Kevin Le |
|
| Gwendolyn Moscoe |
Katherine Miller |
Officers and Board of Directors
LINDA FRED
President
GINGER ERTEL
Treasurer
660-342-5022
gertel@msn.com
CHARLENE HOPE
Secretary
708-783-5933
TRAVIS HUNERDOSSE
Director, Educational Affairs
thunerdo@nmh.org
CARRIE VOGLER
Director, Marketing Affairs
217-545-5394
DESI KOTIS
Director, Professional Affairs
KATHRYN SCHULTZ
Director, Government Affairs
312-926-6961
MIKE WEAVER
Chairman, House of Delegates
815-599-6113
mweaver@fhn.org
ANA FERNANDEZ
Technician Representative
312-926-6980
DAVID TJHIO
Chairman, Committee on Technology
816-885-4649
david.tjhio@cerner.com
BRANDI STRADER
Chairman, New Practitioners Network
217-544-6464
JACOB GETTIG
Editor & Chairman, KeePosted Committee
630-515-7324 fax: 630-515-6958
jgetti@midwestern.edu
SCOTT MEYERS
Executive Vice President, ICHP Office
815-227-9292
scottm@ichpnet.org
Regional Directors
NOELLE CHAPMAN
Regional Director North
312-926-2547
nchapman@nmh.org
LYNN FROMM
Co-Regional Director South
618-391-5539
TARA VICKERY-GORDON
Co-Regional Director South
618-643-2361 x2330
JULIA SAPOZHNIKOV
Student Chapter Liaison
University of IL C.O.P.
sapozhn1@uic.edu
NEHA KAPUR
President, Rockford Student Chapter
University of IL C.O.P.
kapur4@uic.edu
CAROLYN TOY
President, Student ChapterMidwestern University C.O.P.
ctoy59@midwestern.edu
MARIA LAURA ITUAH
President, Student Chapter
Chicago State University C.O.P.
mituah@csu.edu
KIMBERLEE KABBES
President, Student Chapter
Southern Illinois University Edwardsville S.O.P
kikabbe@siue.edu
COURTNEY MAKOWSKI
President, Student Chapter
Roosevelt University C.O.P.
Upcoming Events
Wednesday, June 16 at 3 pm & Thursday, June 24 at 12 pm
Champion Webinar on Blood Clotting Disorders and Factors (Technician-specific)
Wednesday, July 1
Submission Deadline! 2015 Best Practice Award Entries
TBA July Champion
Champion Webinar on Enoxaparin Therapeutic Drug Monitoring in Pediatric Patients
Thursday, July 16
SSHP Night at the Ballpark
Springfield Sliders vs. West Virginia Miners
Springfield Sliders Baseball Club | Springfield, IL
Saturday, July 18th 7:45am-3pm
Habitat for Humanity Women Build
119th & S Union Ave in the West Pullman neighborhood in Chicago
Thursday, September 10 - Saturday, September 12
ICHP 2015 Annual Meeting
Pharmacist & Technician-specific CPE programming
Drury Lane Conference Center | Oakbrook Terrace, IL

Print Entire Issue

.")

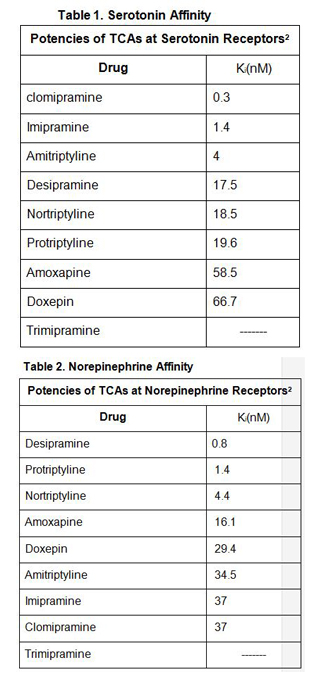
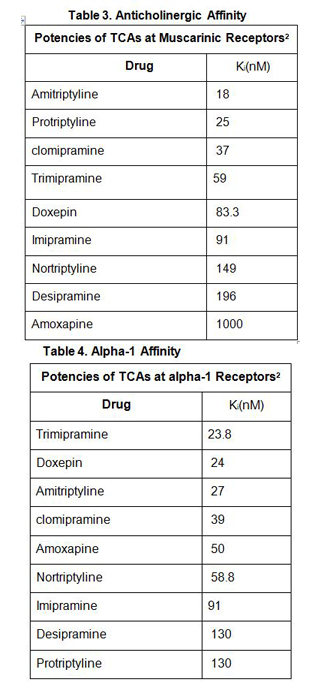
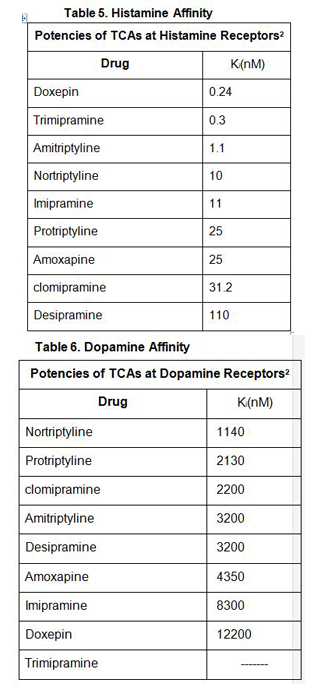
.jpg)
.jpg)

 Visit the ICHP Calendar for the most up-to-date events!
Visit the ICHP Calendar for the most up-to-date events!