Print Entire Issue

KeePosted Info
Features
Lynn Rheinecker Farewell
Get to Know Me and What I Learned – Sarah Sheley
Call for Entries: 2015 Best Practice Award
Nominate the Next ICHP Pharmacist of the Year!
Time to Nominate Our Newest Stars!
ICHP Seeks Nominees for the 2015 Amy Lodolce Mentorship Award
Night at the Ballpark
Columns
President's Message
Directly Speaking
New Practitioners Network
Educational Affairs
Leadership Profile
ICHPeople
Government Affairs Report
Board of Pharmacy Update
Medication Safety Pearl
College Connections
Ronald McDonald House
Knowing the Potential of Our Future Career
Legislative Day
More
Officers and Board of Directors
Welcome New Members!
ICHP Pharmacy Action Fund (PAC) Contributors
Upcoming Events
KeePosted Info
 Illinois Council of Health-System Pharmacists
Illinois Council of Health-System Pharmacists
4055 North Perryville Road
Loves Park, IL 61111-8653
Phone: (815) 227-9292
Fax: (815) 227-9294
www.ichpnet.org
KeePosted
Official Newsjournal of the Illinois Council of Health-System Pharmacists
EDITOR
Jacob Gettig
ASSISTANT EDITOR
Jennifer Phillips
MANAGING EDITOR
Scott Meyers
ASSISTANT MANAGING EDITOR
Trish Wegner
DESIGN EDITOR
Amanda Wolff
ICHP Staff
EXECUTIVE VICE PRESIDENT
Scott Meyers
VICE PRESIDENT - PROFESSIONAL SERVICES
Trish Wegner
DIRECTOR OF OPERATIONS
Maggie Allen
INFORMATION SPECIALIST
Heidi Sunday
CUSTOMER SERVICE AND
PHARMACY TECH TOPICS™ SPECIALIST
Jo Ann Haley
ACCOUNTANT
Jan Mark
COMMUNICATIONS MANAGER
Amanda Wolff
LEGISLATIVE CONSULTANT
Jim Owen
ICHP Mission Statement
Advancing Excellence in the Practice of Pharmacy
ICHP Vision Statement
ICHP dedicates itself to achieving a vision of pharmacy practice where:
- Pharmacists are universally recognized as health care professionals and essential providers of health care services.
- Patients are aware of the training, skills, and abilities of a pharmacist and the fundamental role that pharmacists play in optimizing medication therapy.
- Formally educated, appropriately trained, and PTCB certified pharmacy technicians manage the medication distribution process with appropriate pharmacist oversight.
- Pharmacists improve patient care and medication safety through the development of effective public policies by interacting and collaborating with patients, other health care professionals and their respective professional societies, government agencies, employers and other concerned parties.
- Evidence-based practices are used to achieve safe and effective medication therapies.
- There are an adequate number of qualified pharmacy leaders within the pharmacy profession.
- Pharmacists take primary responsibility for educating pharmacy technicians, pharmacy students, pharmacist peers, other health professionals, and patients about appropriate medication use.
KeePosted Vision
As an integral publication of the Illinois Council of Health-System Pharmacists, the KeePosted newsjournal will reflect its mission and goals. In conjunction with those goals, KeePosted will provide timely information that meets the changing professional and personal needs of Illinois pharmacists and technicians, and maintain high publication standards.
KeePosted is an official publication of, and is copyrighted by, the Illinois Council of Health-System Pharmacists (ICHP). KeePosted is published 10 times a year. ICHP members received KeePosted as a member benefit. All articles published herein represent the opinions of the authors and do not reflect the policy of the ICHP or the authors’ institutions unless specified. Advertising inquiries can be directed to ICHP office at the address listed above. Image disclaimer: The image used in the Pharmacy Tech Topics™ advertisement is the property of © 2015 Thinkstock, a division of Getty Images.
Copyright © 2015, Illinois Council of Health-System Pharmacists. All rights reserved.
Features
Lynn Rheinecker Farewell
by Lynn Rheinecker, P4, University of Illinois at Chicago College of Pharmacy - Rockford Campus
My six-week APPE rotation at ICHP has come to a close. While I am eager to transition towards pharmacy school graduation, it is unfortunate that I have to leave this rotation site. My experience at ICHP was an invaluable one. I had no idea of the behind-the-scenes activities required to make ICHP's mission a reality. During my time here, I have participated and contributed to many of these efforts.
Once the 99th Illinois General Assembly came to session, I created a spreadsheet to monitor pharmacy and other healthcare-related legislation. In particular, ICHP is keeping a close watch on bills associated with Right to Try, the Heroin Crisis Act, and the Pharmacy Practice Act. I am interested to see how these and other bills progress through Congress after I leave.
During my rotation, I also attended an Illinois Board of Pharmacy meeting, where pharmacist participation in out-of-state executions was addressed. After the meeting, I researched, compiled, and submitted relevant sections of the Pharmacy Practice Act, the Standards of Pharmacy Practice, the Pharmacist Code of Ethics, etc., to the ICHP Professional Affairs Committee for review and eventual development of a position statement on this issue.
Additionally, I presented a journal club to the ICHP staff entitled, "What really drives success?" My presentation was based upon ideas in a book by Adam Grant, entitled Give and Take. The staff enjoyed my presentation and all found the material to be applicable to their current positions at ICHP. For this reason, I plan to give the presentation again during my future pharmacy career, because I believe the concepts are relevant to audiences of all career fields and job positions.
My favorite experiences of this rotation were associated with networking. I attended an ICHP Directors of Pharmacy dinner, where I met directors from all over Chicago-land and Rockford. It was valuable to witness the important exchange of ideas and information among these important leaders in pharmacy. Furthermore, I was able to network at the various Legislative Day 101 presentations at surrounding colleges of pharmacy, which I attended with ICHP's Executive Vice President, Scott Meyers. I tried to convey the importance of networking with any student I spoke with at these events.
Well, I guess I have to say good-bye for now and move onto my next rotation site at Freeport Health Network. I want to formally thank the ICHP staff for all of their support and encouragement during my six-week rotation (especially during my residency interviews)! I will miss you all very much! While I might be leaving my duties at ICHP, I plan to remain active in the organization or another ASHP state affiliate throughout the remainder of my pharmacy career.
Get to Know Me and What I Learned – Sarah Sheley
by Sarah Sheley, PharmD Candidate 2015, University of Illinois Chicago College of Pharmacy - Rockford Campus
 Hello all and happy Spring! My name is Sarah Sheley and I am a fourth year pharmacy student at the University of Illinois at Chicago – Rockford campus. I am originally from South Bend, Indiana and received a Bachelor of Science in Biology with Minors in Chemistry and Psychology from Indiana University-South Bend in 2009. I took a year off to work and decided to apply to pharmacy school. I was admitted to UIC-Rockford in Fall of 2011 and have come to call Rockford my home away from home. I currently am working as a pharmacy technician at OSF-St. Anthony Medical Center in Rockford.
Hello all and happy Spring! My name is Sarah Sheley and I am a fourth year pharmacy student at the University of Illinois at Chicago – Rockford campus. I am originally from South Bend, Indiana and received a Bachelor of Science in Biology with Minors in Chemistry and Psychology from Indiana University-South Bend in 2009. I took a year off to work and decided to apply to pharmacy school. I was admitted to UIC-Rockford in Fall of 2011 and have come to call Rockford my home away from home. I currently am working as a pharmacy technician at OSF-St. Anthony Medical Center in Rockford.
Since I started working in the field of pharmacy in 2007 I have shifted between several different settings. I began working as a technician at CVS and moved to Omnicare in 2010, where I worked until I moved to Illinois for pharmacy school. I was hired at OSF St. Anthony in May of 2012 where I am a current employee. Through these different pharmacy experiences, I have been exposed to many different types of patients and healthcare provider communication styles. Through all of these experiences, along with my interactions during pharmacy school, I have developed an understanding that effective collaboration and communication with other members of the healthcare community is vital to providing optimal and safe patient care. I have a strong desire to provide patients with the best care when I graduate and hopefully the skills I have developed along the way will be of benefit.
When I am not working, I am an advocate of volunteer activities and community service projects. I joined several pharmacy organizations my first year at UIC including ICHP. I have participated in many community service and educational events with ICHP from blood pressure and glucose screenings to Legislative Day in Springfield. As an ICHP Mental Wellness Committee member I have helped to organize and collect funds and materials for National Alliance for the Mentally Ill (NAMI) collection drives. I am a strong advocate for increasing awareness about mental illness and attend NAMI meetings occasionally. I have also been a member of APhA, SnAPhA, and AMCP through the last four years at UIC. I also volunteer my time with OSF participating in Keep Northern Illinois Beautiful medication collection drives and mentoring opportunities at the St. Anthony College of Nursing Explore Healthcare Summer Camp. With my interest in mental illness, I planned on pursuing residency training after receiving my PharmD. from UIC in May, but am now looking into hospital pharmacy positions. I enjoy working at OSF St. Anthony and hope to find a staff pharmacy position around the Midwest. I plan on staying involved with community service events with ICHP and NAMI. I would also like to be a preceptor for future pharmacy students in an effort to assist in the growth of future pharmacists.
Outside of school, work and community service projects, I do have several hobbies that I enjoy. When it is warm enough I enjoy going to Rock Cut or Blackhawk Park to hike, canoe or ride my bike. I also enjoy painting, drawing and reading. I have a large family of 5 siblings and my mother back in Indiana, so I visit them as much as possible. They enjoy when I come home because they like my cooking better than my mom's, but don’t tell her!
For the past 6 weeks I have been at the ICHP headquarters on rotation with ICHP Executive Vice President, Scott Meyers. I have had the opportunity to participate in a number of regulatory committee meetings and developed an understanding of the excessive amount of work that goes into the regulations and laws that affect the pharmacy profession. I was involved in the identification and monitoring of many of the legislative documents that were presented at Legislative Day in Springfield this year. I have also had the opportunity to be involved in the process of reviewing continuing education (CE) material for pharmacists and pharmacy technicians. I learned about the ACPE accreditation process and what is involved in developing and presenting CE materials. I attended the ICHP/MSHP Spring meeting in St. Charles, MO with the ICHP staff and experienced what putting on a joint meeting entailed. Needless to say, it was a lot of work! A leadership position, such as Mr. Meyers’, in a pharmacy association is definitely not a walk in the park. There are so many processes that go on behind the scenes to keep the pharmacy profession's interests protected. I have thoroughly enjoyed my time with ICHP staff and have learned things that would not be possible in other pharmacy settings. I definitely will have more appreciation for the provider of the next pharmacy meeting that I attend after being on this rotation.
Call for Entries: 2015 Best Practice Award

The objective of the Best Practice Award program is to encourage the development of innovative or creative pharmacy practice programs or innovative approaches to existing pharmacy practice challenges in health systems within the state of Illinois.
Applicants will be judged on their descriptions of programs and practices employed in their health system based on the following criteria:
- Innovativeness / originality
- Contribution to improving patient care
- Contribution to institution and pharmacy practice
- Scope of project
- Quality of submission
If you have any questions related to the program please contact Trish Wegner at trishw@ichpnet.org.
Previous Winners
2014
Arti Phatak, Pharm.D.; Brooke Ward, Pharm.D., BCPS; Rachael Prusi, Pharm.D.; Elizabeth Vetter, Pharm.D.; Michael Postelnick, BS Pharm, BCPS (AQ Infectious Diseases); and Noelle Chapman, Pharm.D., BCPS
“Impact of Pharmacist Involvement in the Transitional Care of High-Risk Patients through Medication Reconciliation, Medication Education, and Post-Discharge Callbacks”
2013
Nicole Rabs, Pharm.D., Sarah M. Wieczorkiewicz, Pharm.D., BCPS, Michael Costello, PhD, and Ina Zamfirova, BA
“Development of a Urinary-Specific Antibiogram for Gram Negative Isolates: Impact of Patient Risk Factors on Susceptibility”
2012
Kathryn Schiavo, Pharm.D.; George Carro RPh, MS, BCO; Abigail Harper, PharmD, BCOP; Betty Fang, PharmD; Palak Nanavati, PharmD
“Outpatient Oncology Treatment Center Approach to Enhancing Continuity of Care Related to Dispensing Oral Chemotherapeutic Agents”
2011
Fatima Ali, PharmD; Sarah Wieczorkiewicz, PharmD, BCPS; Jill Cwik, PharmD; Robert Citronberg, MD, FACP, FIDSA
“Procalcitonin-Guided Duration of Antimicrobial Therapy for the Treatment of Lower Respiratory Tract Infections”
|
Online entry form: http://www.ichpnet.org/professional_practice/best_practices/
Submission deadline: July 1, 2015
Eligibility
Applicants must be a member of ICHP practicing in a health system setting. More than one program can be submitted by a health system for consideration. Past submissions may be re-submitted if not previously given the award. Any new data should be included.
Instructions for preparing manuscript
Each entry for the Best Practice Award must include a manuscript prepared as a Word document, double-spaced using Times New Roman 12-pitch type. A header with the paper title and page number should appear on each page. The manuscript should not exceed 2000 words in length (not counting references), plus no more than a total of 6 supplemental graphics (tables, graphs, pictures, etc.) that are relevant to the program. Each picture, graph, figure, and table should be mentioned in the text and prepared as a separate document clearly labeled.
The manuscript should be organized as a descriptive report using the following headings:
- Introduction, Purpose, and Goals of the program
- Description of the program
- Experience with and outcomes of the program
- Discussion of innovative aspects of programs and achievement of goals
- Conclusion
Format
Submissions will only be accepted via online submission form. The manuscript will be forwarded to a pre-defined set of reviewers. Please do not include the names of the authors or affiliations in the manuscript to preserve anonymity.
All applicants will be notified of their status within three weeks of the submission deadline. Should your program be chosen as the winner:
- The program will be featured at the ICHP Annual Meeting. You will need to prepare a poster to present your program and/or give a verbal presentation. Guidelines will be sent to the winner.
- You will be asked to electronically submit your manuscript to the ICHP KeePosted for publishing. This program will be accredited for CPE and will require that you complete material for ACPE accreditation.
- You will receive a complimentary registration to the ICHP Annual Meeting, recognition at the meeting and a monetary award distributed to your institution.
Non-winning submissions may also be considered for publication in the ICHP KeePosted, but your permission will be obtained beforehand.
Thank you to PharMEDium for providing a grant for the 2015 Best Practice Award!
|
Nominate the Next ICHP Pharmacist of the Year!
ICHP is looking for the best of the best for the 2015 Pharmacist of the Year Award Recipient! You should recognize some of the previous years’ winners as they have been pharmacy leaders in Illinois and nationally: Stan Kent, Kevin Colgan, Andy Donnelly, Miriam Mobley-Smith, Mary Lee and so many more! One of the earliest recipients of Illinois health-system pharmacy’s highest award, Herb Carlin, served as President of both ASHP and APhA. A feat that has been done by only a very select few!
The ICHP Pharmacist of the Year Award recognizes a pharmacist who has worked in or around health-system pharmacy making substantial and sustained contributions to health-system practice or the profession in general. Below are the criteria for selection. Nominators should send a letter outlining the nominee’s accomplishments in detail to Mary Moody, 2014 Award Recipient and 2015 Selection Committee Chair at mlmoody@uic.edu or Scott Meyers at scottm@ichpnet.org.
Selection Criteria
The Illinois Health-System Pharmacist of the Year Award is given annually, if a recipient is chosen, to an individual of high moral character, good citizenship and high professional ideals, who has made significant contributions affecting the practice of health-system pharmacy throughout the state. These contributions shall have been in the form of sustained exemplary service in health-system pharmacy, or, a single outstanding achievement, or, a combination of accomplishments benefiting health-system pharmacy, and through it, humanity and the public health. They may include accomplishments, achievements or outstanding performance in:
- health-system pharmacy practice,
- health-system pharmacy education,
- health-system pharmacy administration,
- pharmaceutical research or development related to health-system pharmacy,
- pharmacy organizational activity with a definite relationship to health-system pharmacy,
- scientific or professional pharmaceutical writing, e.g., noteworthy articles on pharmaceutical subjects with applicability to health-system pharmacy,
- pharmaceutical journalism related to health-system pharmacy,
- public and/or interprofessional relations activities benefiting health-system pharmacy,
- pharmaceutical law or legislation, professional regulations, standards of professional conduct or pharmacy law enforcement as related to health-system pharmacy practice.
Past Recipients of ICHP’s Pharmacist of the Year Award
1966 F. Regis Kenna *
1967 Louis Gdalman *
1968 C. Charles Lev *
1969 Edward Hartshorn
1970 Herbert Carlin *
1971 Sr. Mary Louise (Matthew) Degenhart
1972 Harland E. Lee
1973 Roger Klotz
1974 Ronald Turnbull
1976 John Lewis
1977 Raphael Jacobson *
1978 Terry Trudeau *
1979 Merrikay Oleen
1980 Sr. Margaret Wright
Ernie Steinbaugh **
1981 Karen Nordstrom
1982 Mary Maranti *
1983 E. Clyde Buchanan
1984 David Vogel *
1985 William Wuller
1986 LeRoy Hayes *
1987 Max L. (Mick) Hunt
1988 Marcia Palmer
1989 Lee S. Simon
1990 Edna Dooley
1991 Scott A. Meyers
1992 Kenneth Witte
1993 Kevin Colgan
1994 Alan Weinstein
1995 Edward Donnelly
1996 Bruce Dickerhofe
1997 Steven E. Marx
1998 Janet L. Teeters *
1999 James Dorociak
2000 Robert Hoy
2001 Jacqueline Kessler
2002 Andrew Donnelly
2003 Mary Ann Kliethermes
2004 Michael Novario
2005 Miriam Mobley-Smith
2006 Jan Keresztes
2007 Avery Spunt
2008 Stan Kent
2009 Michael Fotis
2010 Mary Lee
2011 Michael Weaver
2012 Patricia Wegner
2013 Ann Jankiewicz
2014 Mary Moody
* deceased
** awarded posthumously
Time to Nominate Our Newest Stars!
New Practitioner Leadership Award Nominees Sought
by Scott A. Meyers, Executive Vice President
ICHP has been blessed with a wealth of young pharmacy practitioners and we’re looking for your nomination of the brightest one to receive the 2015 Illinois Council of Health-System Pharmacists' New Practitioner Leadership Award. The award recognizes an individual whose early accomplishments distinguish them as a future leader in the profession. The candidates should be individuals whose performance demonstrates a high degree of professionalism, leadership, and innovation. Nominations may be submitted to the ICHP office through Thursday, June 18, 2015 by an affiliate chapter or any two individual members of the ICHP. If a nominee is selected to receive the award, it will be presented at the Annual Meeting. Nominees should meet the following criteria:
- Earned his/her first pharmacy degree within the last 10 years,
- Encourage and support ICHP by membership, meeting attendance, and participation*,
- Demonstrate a consistently high level of professional achievement,
- Has developed, is working in or is working towards the development of an innovative practice in Health-System pharmacy practice,
- Exhibit strong leadership qualities, and
- Possess a strong commitment to the advancement of the pharmacy profession.
* Membership in ICHP and volunteer activity within ICHP’s divisions, committees or board of directors are absolute requirements to receive this award.
To apply or nominate someone for this award, please forward a detailed letter of recommendation identifying the specific accomplishments of the nominee with respect to each of the criteria above to ICHP, 4055 N Perryville Road, Loves Park, IL 61111-8653, or email to scottm@ichpnet.org. Nominations for 2015 are due Thursday, June 18, 2015.
Selection of a recipient shall be by the ICHP Board of Directors in a secret ballot. The nominator may be requested to provide additional information to the ICHP Board of Directors to facilitate discussion and selection.
Help us recognize one of tomorrow’s leaders and an outstanding new practitioner of today!
ICHP Seeks Nominees for the 2015 Amy Lodolce Mentorship Award
In 2013, ICHP created the Amy Lodolce Mentorship Award in memorial to Amy Lodolce a University of Illinois at Chicago College of Pharmacy faculty member, who touched the lives of pharmacy students, residents, and colleagues through her passion for teaching and the profession of pharmacy. Throughout her time at the college, Amy oversaw the training of four PGY2 drug information pharmacy residents, all of whom are currently drug information faculty members at various institutions. She worked directly with numerous PGY1 residents and APPE students during their drug information rotations. She also served as a formal mentor to her student advisees and was the advisor of the Phi Delta Chi pharmacy fraternity for many years. As the Assistant Director of the Drug Information Group, Amy served as an informal mentor to other faculty and was quick to help new faculty become oriented and situated. Amy approached being a leader and a mentor with an “open door” policy and would selflessly pause her work to address others’ needs. Students, residents, and faculty were impacted by her dedication as she worked tirelessly to provide them with quality learning opportunities. On August 31st, 2012, Amy passed away at a young age of 38 after a long illness, and this award has been created in her memory. Amy’s dedication and generosity to the profession of pharmacy have positively shaped many pharmacists’ careers, and the memory of her will continue to do so.
Award Criteria:
- The individual nominated to receive this award must be an ICHP pharmacist, associate or technician member in good standing;
- The individual should be an exemplary preceptor, professor and/or mentor of students, residents, pharmacy technicians and/or new practitioners;
- The individual should be a positive role model for pharmacists, pharmacy students and/or pharmacy technicians;
- In order to be considered for the award, individuals must have been nominated using the approved nomination form below;
- More than one person may complete a nomination form for an individual.
Your name(s) (more than one person may nominate):________________________
Person you are nominating:__________________________
- In what capacity have you worked with this individual?
- In what ways do you see this individual working to advance the profession of pharmacy?
- Please provide some examples of ways in which this person is an outstanding role model, mentor or preceptor.
- Please provide some examples in which this person has demonstrated a service to community (outside of job responsibilities).
- How has this individual impacted your career?
Award Process:
- Each spring, a call for nominations will appear in KeePosted.
- The nomination form will be available on the ICHP website: www.ichpnet.org/awards
- Nominations may be received through June 30th of each year and should be sent to the ICHP office.
- The ICHP Executive Committee will review all nominations and select the finalists.
- The ICHP Board of Directors will select a recipient, should one be chosen.
- The award winner will be notified prior to the ICHP Annual Meeting to ensure attendance, and the award will be presented during the awards banquet.
- In the event that there are no suitable nominees for the award, an award will not be presented.
Night at the Ballpark
Wednesday, May 27th, 2015
7:05 pm - 10:00 pm
New Practitioners Network & Pharmacy Directors Network- Night at the Ballpark
Chicago Cubs vs Washington Nationals
7:05 pm
Tickets are $12
Terrace Reserved (OF)
This spring the ICHP New Practitioners Network welcomes the ICHP Chicago-area Pharmacy Directors Network to join them for their annual evening of Cubs baseball, hot dogs, nachos and more at Wriggly Field on May 27th as the Chicago Cubs take on the Washington Nationals at 7:05 p.m. Tickets for seats in the lower level Reserved Terrace Seating are only $12 each but are only available to New Practitioner, Pharmacy Director, Residency Director and Resident members of ICHP and only one ticket may be purchased per member. This year the tickets are all together in five rows of 10 seats! This is an event you won’t want to miss!
Order your ticket below. You will be mailed your ticket within 7-10 days and the deadline for ticket sales will be Wednesday, May 20th. All food and beverage purchases are the individual member’s responsibility at the game. So bring some folding money or your plastic and be ready for some great baseball and outstanding networking! Tickets will go fast this year so click here to order your ticket now!
Columns
 President's Message
President's Message
Interdisciplinary Rounding – Collaboration at the Patient Care Team Level
by Linda Fred, ICHP President
Here at Carle, we have been working for about six months on redesigning how our hospitalist service’s multidisciplinary rounding teams function. It has been a very interesting and challenging experience. I’d like to just ramble for a few paragraphs about some of the history and evolution of multidisciplinary rounding services that I’ve seen over the course of my career.
My first exposure to pharmacist decentralization and rounding was about 25 years ago. At the time, I was working primarily second shift and I wasn’t doing much rounding personally – because in a community hospital with community-based physicians, not much rounding happened in the evening. In fact, the hospital wasn’t doing much in the way of formalized multidisciplinary rounding at all. The pharmacists were decentralized and available on the floor, on both first and second shift (although scaled back in the evenings), but rounding with a team was happening very minimally. Again, with community based providers, formalizing something like interdisciplinary rounds presents additional challenges.
A lot of the work at that time was still distribution focused, too. A pharmacist or a tech would visit the units, pick up orders, and determine if there were any issues (e.g., missing doses and similar things). If we had a problem with an order, we might track the provider down in person to have that conversation. That was always so much easier than having to page them after they left. There were consult orders for things like discharge education, dosing, and interactions/adverse events. I feel like we were loosely considered part of a provider team. They certainly missed us when we weren’t there. But a lot of the collaboration was almost an afterthought. The patient would have a problem, and the first time we would hear about it was after everything else was exhausted, and someone would say, “Maybe we should ask pharmacy”. I think a lot of that was driven by the fact that the pharmacists weren’t consistently present at the time care decisions were being made. So the providers became very used to making the decisions with the expectation that if there was a pharmacy issue, we would come to them. And, that’s pretty much how it worked. I’m sure academic centers were farther along in the evolution of clinical practice – but in community hospitals, this wasn’t an uncommon model.
About 20 years ago I relocated to Urbana and began working at Carle. One of the biggest differences between this environment and my last one was the close affiliation – and eventually joint ownership – of the physician practice and the hospital. The second thing that became a big driver of multidisciplinary rounding was the development of hospitalist services. Hospitalists become masters at navigating hospital systems. They rapidly began to understand the interconnectivity of all the services and how they all have to work together to successfully achieve the discharge criteria that will move a patient to the next level/site of care. Having a patient spend another day in a bed because we couldn’t facilitate their DME needs, or the physical therapist’s assessment didn’t get scheduled, or the case manager didn’t know it was a nursing home placement, or the home infusion pharmacy didn’t find out until 6:00 p.m. that they needed a prior authorization on a drug or that the patient needed teaching on a home pump – ties up the bed, dissatisfies the patient and the family, and costs the hospital money. Hospitalists are often the biggest and best advocates for having a full team rounding approach because they see first-hand the value of having all services in the same room at the same time to problem-solve for the patient.
I’ve seen several iterations of “rounding”, sometimes based on convenience or geography, sometimes based on provider preference. I don’t know that one is inherently better than another. Teaching services often physically round on patients by walking room to room and having someone (often a resident or student) present the case. The team discusses that day’s issues and updates the plan of care. Each service brings up relevant issues, the residents and students get quizzed a little, and decisions are made as a group. Some services do more of a table-top version of rounds sometimes called “care conferences”. Rather than physically moving room to room, the group congregates in a conference room and rounds are conducted by the team with the medical record, if not the patient, in front of them. Some rounds are “global” patient rounds, where all patient care needs are discussed; some are service specific, such as ID. Some rounds are very focused on discharge planning needs and patients not ready for discharge are rounded on separately. The type of rounds, their structure, or the location are less important than the philosophy of having the input of an entire team of providers, sharing insights specific to their areas of expertise, and driving the care of the patient in a coordinated manner.
One rewarding aspect of our current redesign project is the enthusiastic support we are receiving from the medical staff. The pharmacy profession is maturing to the point where we are respected and desired members of that collaborative team. It is especially gratifying to have our Hospitalist Providers say things like, “The new model can’t work unless we have the entire team there to support our physicians. We need therapy services, case management, nursing, pharmacy – everyone at the table.”
I had a provider say to me today how appreciative he is of the strength of our pharmacy services. He said during physician recruitment, he tells prospective new providers that we have great pharmacy services, Board Certified staff, and that pharmacy is one area he never has to worry about. His wish list, as we met today to talk about current and future services, was more clinical involvement of the pharmacists in care delivery decisions.
I’ve worked my entire career in community hospitals and this has been my dream – that pharmacists are sought after; that we are recognized for our skills; that we are appreciated as more than just the people who provide the physical product. We are enjoying a wealth of opportunities right now in collaboration with multidisciplinary teams. I hope that my experiences at Carle are being replicated elsewhere – and that my fellow pharmacists are making the most of them.
 Directly Speaking
Directly Speaking
Be All That You Can Be: In Your Life
by Scott A. Meyers, Executive Vice President
“Be all that you can be” was the recruiting slogan for the US Army from 1980-2001 and was recently voted by Advertising Age Magazine as the second greatest jingle in advertising history.¹ It was five words that transformed the new Army and told young men and women that it was looking for a new kind of soldier. A more educated young person that could use the Army as a stepping stone to good career and a better life.
That slogan is a great slogan for any pharmacy student, new practitioner and new pharmacy technician to this day. Actually it is a great slogan for every living being, if you think about it! Who wants to be the least that you can be?! I know some people who treat work that way, but then, they aren’t happy nor are they going anywhere in the near future, career-wise anyway! But I digress, Pharmacy is a great career with clean surroundings, a good wage and good benefits. More importantly, you spend your days helping people!
Yes, there are specific requirements to become a pharmacist, not everyone is suited for the job and yes, the requirements for becoming a pharmacy technician continue to be raised as the profession and society see the need for well-trained and accountable support staff. So it’s not as easy to become either as it was in the 1970’s, 80’s and even the 90’s, when I was working on the front lines. But the lessons I learned back then, still apply today. You need to “Be all that you can be!”
What do I mean in saying “Be all that you can be!”? I think it means never passing up a chance to learn something new. When a new project or service is initiated in your department, volunteer to help get it started. When the pharmacy director asks who would like to serve on a hospital committee (I know, most of the time, the director has someone specific in mind), go for it. Or better yet, ask if you can shadow the current department member on a specific committee for one meeting or more. You will be surprised what you can learn not only about what the committee is doing, but often you can learn why you and your colleagues in the pharmacy are doing what you are doing the way you do!
But there’s more! Make a conscious effort to attend a state or local pharmacy association meeting, if there is one around. If none are close, consider visiting a former classmate at their facility on one of your days off for a tour and some idea sharing. You don’t have to be a boss to do this, and it will demonstrate to your boss that you have some personal initiative. That doesn’t mean you need to be a (pardon the expression) suck up, but showing initiative and volunteering to learn something new is always a positive attribute. Most people don’t care for change and often resist it for as long as they can. Being an early adapter or an innovator will make you a valuable commodity in the eyes of good leaders.
Students and new practitioners need to understand that pharmacy is more than a job. It’s not a clock in and clock out when you’re scheduled kind of thing. Pharmacy is more of a “leave only when the job’s done and there are no loose ends” kind of profession. It’s a never leave your colleagues in the lurch profession. Because it is a profession! And we should never hear “It’s not my job” in the pharmacy unless it is immediately accompanied by “But I will get the person who can make that happen!” You see, if you’re looking for someplace to make a lot of money, with little responsibility and no requirement for accountability, you’ve picked the wrong profession or worse yet, job! (If you think any position in the pharmacy is a job, you’ve already made a bad decision!) Yes, you should be able to provide for your family, but health care in general and pharmacy specifically for us, should be patient-focused at all times. And if you continuously learn new things and take on new responsibilities, at the least you won’t be bored and who knows, maybe it can lead to greater things than you ever imagined? If you “Be all that you can be” every day and refuse to accept the position you’ve taken as the only tasks you should perform, I promise, you will have a rewarding career and will always feel good about pharmacy! Be all that you can be!
Reference:
New Practitioners Network
A Small Step To Help a Big Cause
by Bibek Shrestha, PharmD, University of Illinois at Chicago College of Pharmacy
 On a cold January day, the New Practitioners Network (NPN) of Illinois Council of Health-System Pharmacists (ICHP) collaborated on a volunteer event with ‘Feed My Starving Children’ (FMSC), a non-profit organization whose objective is to work towards eliminating starvation in children all around the world.
On a cold January day, the New Practitioners Network (NPN) of Illinois Council of Health-System Pharmacists (ICHP) collaborated on a volunteer event with ‘Feed My Starving Children’ (FMSC), a non-profit organization whose objective is to work towards eliminating starvation in children all around the world.
According to the United Nations World Food Programme (WFP), 3.1 million children under the age of five die of poor nutrition each year. As students and practitioners in the healthcare field, we are well aware of the importance of nutrition in the mental and physical development during the early stages of life. Watching the reports in the media about child hunger and looking at the images of severely underweight children in the third world countries has always been painful to me. As a passionate believer of abolishing child hunger, I signed up for this volunteer event to play my part to reduce child hunger.
 The volunteer event started at 11:30am with a brief introduction about FMSC. After the introduction, we were given a basic outline of our volunteer duties. The goal was to pack MannaPackTM rice packets, a specially designed food mixture developed by FMSC that contain proportions of dry rice, extruded soy nuggets, dehydrated vegetables, blend of vitamins and minerals, and a vegetarian flavoring. Volunteers were divided into multiple groups and each group was assigned a specific task. My group was assigned to refill rice and dry soy in their respective stock bins. Other groups were delegated duties that included pouring, packaging, and replenishing ingredients at the six stations. Each of the six stations had 6-7 volunteers, some of whom were kids. Each station volunteer was assigned to measure out one ingredient and pour it into the MannaPackTM packet, which was then sealed and packed in boxes. Each box of MannaPackTM rice contained 36 individual packets serving 216 meals. Every time a group completed a box of MannaPackTM rice, the group members shouted-out their chosen mantra, energizing the rest of the volunteers. These boxes were then sent by FMSC to missionary partnership humanitarian relief organizations around the world, and were ultimately distributed to kids in orphanages, schools, refugee camps, malnourishment centers, and clinics. On this specific day, the packed boxes were set to leave for kids in Madagascar.
The volunteer event started at 11:30am with a brief introduction about FMSC. After the introduction, we were given a basic outline of our volunteer duties. The goal was to pack MannaPackTM rice packets, a specially designed food mixture developed by FMSC that contain proportions of dry rice, extruded soy nuggets, dehydrated vegetables, blend of vitamins and minerals, and a vegetarian flavoring. Volunteers were divided into multiple groups and each group was assigned a specific task. My group was assigned to refill rice and dry soy in their respective stock bins. Other groups were delegated duties that included pouring, packaging, and replenishing ingredients at the six stations. Each of the six stations had 6-7 volunteers, some of whom were kids. Each station volunteer was assigned to measure out one ingredient and pour it into the MannaPackTM packet, which was then sealed and packed in boxes. Each box of MannaPackTM rice contained 36 individual packets serving 216 meals. Every time a group completed a box of MannaPackTM rice, the group members shouted-out their chosen mantra, energizing the rest of the volunteers. These boxes were then sent by FMSC to missionary partnership humanitarian relief organizations around the world, and were ultimately distributed to kids in orphanages, schools, refugee camps, malnourishment centers, and clinics. On this specific day, the packed boxes were set to leave for kids in Madagascar.
 At the end of our two hour shift, FMSC tallied the boxes and reported that we had packed 113 boxes of MannaPackTM rice, equivalent to 24,408 meals - enough to feed approximately 67 children for a year. With the help of donors and volunteers, FMSC is able to keep the production cost of each meal at an amazingly low 22 cents. Being able to help so many kids in so little time provided me with a great sense of satisfaction. I was also amazed to see children as young as five years old volunteering at this event. The event had provided a wonderful opportunity for the parents to engage their children in developing compassion for the underprivileged while learning to work in a team.
At the end of our two hour shift, FMSC tallied the boxes and reported that we had packed 113 boxes of MannaPackTM rice, equivalent to 24,408 meals - enough to feed approximately 67 children for a year. With the help of donors and volunteers, FMSC is able to keep the production cost of each meal at an amazingly low 22 cents. Being able to help so many kids in so little time provided me with a great sense of satisfaction. I was also amazed to see children as young as five years old volunteering at this event. The event had provided a wonderful opportunity for the parents to engage their children in developing compassion for the underprivileged while learning to work in a team.
After the event, a few of the ICHP members, including students and new practitioners met at a nearby restaurant, where we had an open discussion about the changing role of pharmacists under the Affordable Care Act (ACA), while enjoying our meals. As health-systems work towards preventing hospital readmissions, pharmacists play a crucial role to improve health outcomes. For example, some retail pharmacy chains are now contracting with hospitals to perform medication patient counseling and medication reconciliation with patients after discharge.
On my way back home from this event, I had a sense of joy and satisfaction that was palpable. Giving back to our community helps people in need, while at the same time, it builds confidence and compassion. This volunteer event was a small step towards a big goal, the goal to eliminate starvation in children all around the world.
Educational Affairs
ICHP 2015 Spring Meeting Poster Abstracts
PLATFORM PRESENTATIONS
- Effect of new services and related marketing on employee e-prescription capture rate in an academic medical center retail pharmacy
- Vancomycin use and monitoring following rapid testing of bloodstream cultures for Staphylococci and oxacillin susceptibility
ORIGINAL
- Erectile Dysfunction Medication Use in Veterans Eligible for Medicare Part D
- Descriptive study evaluating the integration of medication management services in a hospital based wound healing center
- Improving the Care of Infants with Neonatal Abstinence Syndrome (NAS). Impact of a standardized methadone dosing algorithm on NAS
- Evaluating Pharmacists’ Role in Hepatitis C Treatment
- Evaluation of Therapeutic Enoxaparin Anti-Xa Level Monitoring in the Obese Patient Population: A Retrospective Chart Review
- Impact of Pharmacists on Interdisciplinary Team Rounding
- Guideline compliance and clinical outcomes among patients with Staphylococcus aureus bacteremia with and without Infectious Diseases consultation
- Comparison of the safety and efficacy for single and multiple tablet first-line regimens for Human Immunodeficiency Virus (HIV)
ENCORE
- Use of raltegravir in HIV-infected pregnant women: a case series and review of the literature
- Pharmacy consults on adult hospitalized patients with delirium
- Outreach Program for Members of An ASHP Chapter
- Impact of PharmD clinic referrals on hemoglobin A1c in an outpatient clinic
STUDENT
- Adherence to IDSA guidelines for the treatment of Uncomplicated Cystitis in a Community Hospital Emergency Department
- Staffing Requirements of PGY1 Pharmacy Residencies in Large Hospitals and PGY2 Pediatric Residencies
- The Forgotten Transition of Care: Discharge Protocol from Hospital to Community Pharmacy
- A Business Plan to Enhance Access to Quality Care among Veterans in Rural Communities
- Peer Review Opportunities and Training in Illinois Residency and Fellowship Programs
- Hedgehog and Tyrosine Kinase Inhibitors for Treating Breast Cancer
- A retrospective chart review of chronic pain medication management
ICHP Poster Presentations - Platform Presentation #1
Category: Original Research – Complete
Title: Effect of new services and related marketing on employee e-prescription capture rate in an academic medical center retail pharmacy
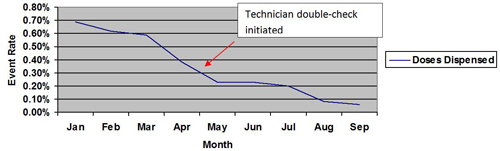
Purpose: The purpose of this study is to investigate the effect of new service offerings and related marketing on e-prescribing capture rate of employee prescriptions at the University of Chicago Medicine Duchossois Center for Advanced Medicine Retail Pharmacy.
Methods: In April of 2013, 1673/3246 (51.5%) of e-prescriptions ordered by University of Chicago Medicine providers for patients with the University of Chicago Health Maintenance Organization Plan were sent to the Duchossois Center for Advanced Medicine Retail Pharmacy. In an effort to increase this capture rate, Department of Pharmacy Leadership established mail order services in May of 2013, installed a lockbox for prescription drop off outside of pharmacy hours of operation in July of 2013, and created a gift card program for new or transferred prescriptions in December of 2013. Marketing related to these initiatives included “table tents” and flyers in high traffic areas of the medical center campus, new employee orientation materials, emails, elective computer based training modules during health benefit enrollment, and organization newsletter articles.
Results: A statistical process control chart of monthly e-prescribing capture rate of prescriptions for patients enrolled in the University of Chicago Health Maintenance Organization Plan dating to January of 2013 revealed no statistically significant increases as of July of 2014.
Conclusions: Despite new service offerings and related marketing, the University of Chicago Medicine Duchossois Center for Advanced Medicine Retail Pharmacy was unsuccessful in increasing e-prescribing capture rate of employee prescriptions. Novel approaches to increasing this capture rate should be further explored.
Authors: Bryan C. McCarthy Jr., Pharm.D., M.S., BCPS Interim Director of Ambulatory Care Pharmacy Services The University of Chicago Medicine, Magdalene Ladas, Pharm.D. Pharmacy Manager, DCAM OutPatient Pharmacy The University of Chicago Medicine (*?)Jennifer Tryon, Pharm.D., M.S. Executive Director of Pharmacy The University of chicago Medicine
ICHP Poster Presentations - Platform Presentation #2
Category: Student Research - Complete
Title: Vancomycin use and monitoring following rapid testing of bloodstream cultures for Staphylococci and oxacillin susceptibility
Purpose: Upon implementing rapid diagnostic testing for bloodstream cultures, we evaluated reporting of Staphylococci and oxacillin susceptibility along with differences in vancomycin duration and monitoring.
Methods: The GeneXpert SA/MRSA (PCR) test for S. aureus and the mecA gene indicating oxacillin resistance was implemented in the local microbiology laboratory during July 2014. Charts of patients with blood cultures positive for S. aureus and Coagulase Negative Staphylococci (CONS) were reviewed from before (n=100) and after implementation (n=54). Factors analyzed included empiric antibiotics, time from blood culture to reporting result, therapy change, and whether a vancomycin level was drawn. Summary of results were compared using Students t-test for continuous variables and Fisher’s exact for nominal data
Results: With S. aureus, the mean time to reporting oxacillin susceptibility prior to PCR testing was 61.1 hours, compared to 18 hours after. For confirmation of CONS, the time decreased from 47.9 hours prior to PCR to 27.5 hours after. When applicable, the time to vancomycin discontinuation for S. aureus was reduced from 73.2 hours prior to PCR and 54.8 hours after (p=0.04). In CONS that value was unchanged at 42.7 vs. 47.4 hours. Before PCR testing, 64% of patients on vancomycin had a serum concentration drawn compared to 54% after (p=0.23).
Conclusion: PCR testing significantly reduced time to reporting of Staphylococci and oxacillin susceptibility in bloodstream cultures. Although the time to discontinuing vancomycin for S. aureus decreased when appropriate, a change in the rate of serum concentration monitoring could not be detected in this sample overall.
Authors: Michael Santini, PharmD Candidate - Southern Illinois University Edwardsville Julie Podlasek, PharmD - Antimicrobial Stewardship Coordinator, Department of Pharmacy, Memorial Medical Center Jerry Lawhorn, BS - Microbiology Supervisor, Department of Laboratory Medicine, Memorial Medical Center Scott J. Bergman, PharmD, BCPS - Associate Professor, Department of Pharmacy Practice, Southern Illinois University Edwardsville
ICHP Poster Presentations - Original #1
Category: Original Research – Complete
Title: Erectile Dysfunction Medication Use in Veterans Eligible for Medicare Part D
Purpose: Medicare Part D covered erectile dysfunction (ED) medications during 2006 and inadvertently in 2007 and 2008. The objective of this study was to characterize prescription ED medication use among veterans who were dual eligible for Veterans Affairs (VA) pharmacy benefits and Medicare Part D. This study evaluated the ED medication use before, during, and after the dual coverage period for ED prescriptions and whether Medicare coverage affected ED prescriptions filled at VA.
Methods: A sample of veterans >66 years who received at least 1 prescription for an ED medication between 2005-2009 were included in this retrospective cohort study. Veterans were categorized by ED medication claims: VA only, Part D only, or dual users of both VA and Part D. The number of unique patients, total number of tablets, and number of prescriptions were obtained.
Results: A total of 25,974 veterans filled a prescription for an ED medication from 2005-2009. The majority of veterans (85.6%) utilized only VA benefits for their ED medications, 11.2% utilized Medicare Part D benefits exclusively and 3.2% were dual users. In 2006, with the inception of Medicare Part D, the total number tablets dispensed (-53.2%) and patients filling ED medications (-38.5%) overall decreased from 2005. In October 2007, ED prescription use began to recover towards the initial baseline.
Conclusions: In this sample of veterans, there was a reduction in ED medication filled prescriptions and unique patients during this period of dual-eligibility as VA benefit utilization decreased without a compensating utilization of Medicare benefits.
Authors: Samantha H. Spencer PharmD*; College of Pharmacy, University of Illinois at Chicago, Chicago, IL Katie Suda PharmD, MS; Center for Innovation in Complex Chronic Healthcare, Hines VA Hospital, Hines, IL; College of Pharmacy, University of Illinois at Chicago, Chicago, IL Bridget M. Smith PhD; Center for Innovation in Complex Chronic Healthcare, Hines VA Hospital, Hines, IL; Feinberg School of Medicine, Northwestern University, Chicago IL Zhiping Huo MS; Center for Innovation in Complex Chronic Healthcare, Hines VA Hospital, Hines, IL Lauren Bailey MS; Center for Innovation in Complex Chronic Healthcare, Hines VA Hospital, Hines, IL; School of Public Health, University of Illinois at Chicago, Chicago, IL Kevin T. Stroupe PhD; Center for Innovation in Complex Chronic Healthcare, Hines VA Hospital, Hines, IL; Stritch School of Medicine, Loyola University Chicago, Maywood, IL
ICHP Poster Presentations - Original #2
Category: Original Research – In Progress
Title: Descriptive study evaluating the integration of medication management services in a hospital based wound healing center
Purpose: Pharmacists are trained to work and collaborate in a variety of settings with different healthcare professionals. The role of the clinical pharmacist in a non-traditional clinical setting such a wound healing center has not been studied. The objective of this study is to report the results of the integration of medication management services (MMS) led by pharmacist in a non-traditional clinic setting and to describe the type of interventions done during the study period
Methods: A retrospective chart review of the patients that received MMS by the pharmacist or pharmacy students at least once between January 2013 and December 2013 was performed. Medication related problems (MRP), adverse drug events (ADE), potential adverse drug events (pADE), interventions and recommendations provided were collected. Results: Results and conclusions are pending.
Conclusion: Results and conclusions are pending.
Authors: *Julio A. Rebolledo, Pharm.D.,BCPS, AE-C Assistant professor, Pharmacy Practice Midwestern University Chicago College of Pharmacy Norwegian American Hospital; Charlene A. Hope, Pharm.D., BCPS, CPHQ, CPPS Chicago Market Pharmacy Quality and Safety Manager MacNeal Hospital-Tenet Healthcare; Angeles M. Valdes, DPM, FACLES, FAPWCA Medical Director, The wound Healing Center Norwegian American Hospital
ICHP Poster Presentations - Original #3
Category: Original - Research In Progress
Title: Improving the Care of Infants with Neonatal Abstinence Syndrome (NAS). Impact of a standardized methadone dosing algorithm on NAS
Purpose: A quality improvement project to determine if intervening with a weight based methadone dosing algorithm can impact hospital length of stay.
Methods: Chart review of a pre-intervention group of infants treated for NAS prior to algorithm implementation compared to a post intervention group of infants. ICD 9 code 779.5 neonatal abstinence syndrome, and gestational age was used to identify subjects for inclusion. A questionnaire will assess compliance with algorithm. T-test statistical analysis will be used to determine significance of primary objective. Study period is June 2011 until February 2015. Total of 57 patients included in data analysis
Results: Subjects treated with algorithm should average a 20 % decrease in length of stay, and receive more non-pharmacologic treatment. Overall compliance goal with algorithm is 80%. Efforts to decrease methadone exposure using a dosing algorithm can impact length of stay, and increase the use of non-pharmacological treatment strategies. Compliance with algorithm will be measured to ensure reproducible results.
Authors: Ann M Corkery, PharmD* Jennifer Mitchell, PharmD
ICHP Poster Presentations - Original #4
Category: Original - Research In Progress
Title: Evaluating Pharmacists’ Role in Hepatitis C Treatment
Purpose: The primary purpose of this project is to survey providers (pharmacists, physicians, nurses) across VA facilities in the nation to characterize pharmacists’ role in managing hepatitis C patients.
Methods: Two surveys were designed to evaluate pharmacists’ involvement and duties in a hepatitis C clinic. Surveys for providers and pharmacists consisting of 11 questions and 13 questions, respectively, were developed. Both surveys were compiled on SurveyMonkey® using skip logic. Surveys were open for 7 weeks from December 4, 2014 until January 23, 2015. A pharmacist’s survey link was emailed to the Clinical Pharmacists and Hepatitis C Pharmacists groups. A provider’s survey link was emailed to the Hepatitis C Clinicians and Coordinators groups. In order to reach out to all providers, a request was made to the pharmacists groups to forward the provider’s survey link to providers who are either working with them or associated with GI/Liver (Hepatitis C) clinics. A reminder to complete the survey was sent at the beginning of the sixth week. Data from survey evaluations will be analyzed and presented at the ICHP Spring Meeting.
Results: In progress
Authors: Kushal Y. Shah*, PharmD; Sue Kim, PharmD, BCPS; Ursula C. Patel, PharmD, BCPS AQ-ID; Andrea M. Mendyk, PharmD, BCPS
ICHP Poster Presentations - Original #5
Category: Original - Research In Progress
Learning Objective: Describe if dosing enoxaparin based upon ABW achieves targeted therapeutic anti-Xa levels in the obese patient population.
Title: Evaluation of Therapeutic Enoxaparin Anti-Xa Level Monitoring in the Obese Patient Population: A Retrospective Chart Review
Purpose: For the obese patient population, guidelines suggest monitoring of low molecular weight heparins with an anti-Xa assay to ensure therapeutic anticoagulation. However, it’s unknown if dosing based upon actual body weight (ABW) per the product instructions, achieves therapeutic anticoagulation in this patient population. The purpose of this study was to evaluate if dosing enoxaparin based upon ABW achieved targeted therapeutic anti-Xa levels for obese patients.
Methods: This retrospective chart review evaluated obese patients treated with therapeutic enoxaparin at the University of Chicago Medicine between 2009 and 2014. The primary endpoint evaluated the percentage of patients that achieved a therapeutic anti-Xa level of 0.6 ? 1 IU/ml on therapeutic enoxaparin at steady state, when dosed upon ABW. Secondary objectives included evaluation of anticoagulation based upon BMI weight stratifications, and if secondary dose adjustments, based upon anti-Xa level results, achieved therapeutic anticoagulation. Patients were identified with medication use reports and electronic medical record abstraction. The study included obese adult patients who received therapeutic enoxaparin and had an anti-Xa level drawn at steady state. Patients were excluded if they were pregnant, had renal dysfunction, were not dosed based upon ABW, or were a burn or bariatric surgery patient. Data collected included patient demographics, enoxaparin regimen, anti-Xa collection time and results, and thrombotic or bleeding occurrences. The baseline patient characteristics and primary endpoint were evaluated using descriptive statistics. A multi-variant regression analysis was completed to determine confounding variables for the primary objective. Secondary outcomes were evaluated with descriptive statistics, chi-squared test, or Fisher’s exact test.
Authors: Luke Jeffrey Hvass*, PharmD, Doctorate of Pharmacy, Creighton University School of Pharmacy, University of Chicago Medicine, PGY-2 Internal Medicine Pharmacy Resident; Hailey Anderson, PharmD, BCPS, University of Wisconsin Madison School of Pharmacy, University of Chicago Medicine, Clinical Pharmacist Specialist, Internal Medicine
ICHP Poster Presentations - Original #6
Category: Original - Research In Progress
Learning Objective: The objective of this study is to describe the impact of the pharmacist during interdisciplinary team rounding.
Title: Impact of Pharmacists on Interdisciplinary Team Rounding
Purpose: Through the Affordable Care Act, Medicare reimbursement is, in part, based on performance, patient satisfaction scores, and reduced readmissions. The American Society of Health System Pharmacists' Pharmacy Practice Model encourages pharmacists to practice at the top of their license as health care providers in direct patient care. Therefore, an interdisciplinary team rounding model developed at our hospital as a way to improve patient healthcare. Using a pharmacist training and expertise more effectively at the bedside helps drive this change. The purpose of this study was to evaluate the contribution of the pharmacist to the interdisciplinary team. The anticipated benefits include increased pharmacist interventions, decreased length of stay, and decreased readmissions.
Methods: This descriptive study was conducted from 6/1/2014 through 12/31/2014 at Kishwaukee Hospital in DeKalb, Illinois. Patients over 18 years of age admitted to the hospitalist service and randomly assigned to the rounding wing of the hospital were included in the study. Intervention data from the pharmacists in the pilot study was collected using Truven surveillance software. Results and Conclusions Final results and conclusions are pending data analysis.
Authors: Virginia J Nash* PharmD BCPS University of Illinois at Chicago Pharmacist Kishwaukee Hospital Kristi Stice PharmD BCPS St. Louis College of Pharmacy Clinical Coordinator Kishwaukee Hospital
ICHP Poster Presentations - Original #7
Category: Original - Research In Progress
Learning Objective:To evaluate the effect of Infectious Disease consultation on the appropriate management of Staphylococcus aureus bacteremia and resulting clinical outcomes.
Title: Guideline compliance and clinical outcomes among patients with Staphylococcus aureus bacteremia with and without Infectious Diseases consultation.
Purpose: Bacteremia caused by Staphylococcus aureus is associated with significant mortality in affected patients. Previous studies have shown that Infectious Disease consultation (IDC) for patients with Staphylococcus aureus bacteremia (SAB) results in improved evaluation and treatment as well as lower rates of complicated infections, morbidity, and mortality. The purpose of this study was to evaluate the effect of IDC on the appropriate management of SAB and resulting clinical outcomes to potentially support an automated IDC for all patients with SAB in the future.
Methods: This retrospective chart review examined patients with SAB at the University of Chicago Medicine from December, 2012, through September, 2014. The primary outcome compared adherence to IDSA guideline recommendations as a composite between patients who received IDC and those who did not; components included echocardiography, removal of implanted prostheses/catheters, follow-up blood cultures, initiation of appropriate antimicrobial therapy, and de-escalation of therapy when appropriate. Secondary outcomes evaluated adherence to each individual component of the primary outcome, as well as clinical outcomes, such as time to microbiologic clearance, recurrence of bacteremia within eight weeks, all-cause in-hospital mortality, and length of stay. Patients were identified with an epidemiology report from the microbiology lab. Data points were obtained through electronic medical record review. This study included patients who were at least 18 years old and had Staphylococcus aureus isolated from at least one blood culture. Patients were excluded if they refused appropriate therapy, left the hospital against medical advice, or were found to be noncompliant with antibiotic therapy at follow up.
Authors: Kevin Buehrle, PharmD* PGY2 Internal Medicine Pharmacy Resident University of Chicago Medicine Natasha Pettit, PharmD, BCPS (AQ-ID) Infectious Disease Pharmacotherapy Specialist University of Chicago Medicine Zhe Han, PharmD, BCPS Infectious Disease Pharmacotherapy Specialist University of Chicago Medicine Jennifer Pisano, MD Infectious Disease Specialist University of Chicago Medicine
ICHP Poster Presentations - Original #8
Category: Original - Research In Progress
Learning Objective: Describe the differences in safety and efficacy between single and multiple tablet regimens for the treatment of HIV.
Title: Comparison of the safety and efficacy for single and multiple tablet first-line regimens for Human Immunodeficiency Virus (HIV)
Purpose: The primary objective of this study is to determine if a single tablet regimen (STR) is associated with increased virologic suppression compared to first-line multi-tablet regimens (MTR) (Atripla/Complera/Stribild vs. Truvada/Reyataz/Norvir, Truvada/Prezista/Norvir or Truvada/Isentress). The secondary goals are to evaluate patient reported adherence, determine if STR or MTR were associated with increased side effects requiring change in therapy, evaluate development of resistance between the study groups, and evaluate maintained virologic suppression in each group in patients with a history of incarceration.
Methods: This is a retrospective chart review study approved by the Institutional Review Board at the University of Illinois Hospital and Health Sciences System. The hospital’s electronic medical record was used to identify patients in one of the Community Outreach Intervention Project clinics or the Family Center for Infectious Diseases clinic who were prescribed one of the antiretroviral (ARV) study regimens between July 2010 and August 2013. Demographic information collected includes: age, gender, ethnicity, and mode of HIV transmission/risk factors. Safety will be assessed during the initial visit and every 6 months by collecting patient reported side effects, laboratory side effects (e.g., SCr, AST/ALT, fasting blood glucose, fasting lipid panel, bilirubin, and CPK). Efficacy will be assessed by collecting baseline CD4, CD4%, and viral load at baseline and every 6 months when available. Adherence will be assessed by collecting patient-reported adherence, refill history, ARV resistance, ARV history, number of pills in ARV regimen, reason for discontinuation or change in ARVs, and frequency of ARV regimen (once vs. twice daily).
Authors: Whitney Dickson, PharmD*, Melissa Badowski, PharmD, Andrew Merker, PharmD, Tommy Chiampas, PharmD, Renata Smith, Rodrigo Burgos, PharmD University of Illinois at Chicago
ICHP Poster Presentations - Encore #1
Category: Encore
Title: Use of raltegravir in HIV-infected pregnant women: a case series and review of the literature
Purpose: In the treatment of antiretroviral (ARV) naïve pregnant women, raltegravir (RAL) is only recommended as an alternative therapy due to lack of safety and efficacy data of RAL in pregnant women. Previous studies of RAL in the use of preventing perinatal transmission have noted rapid suppression of RNA viral loads and well-tolerance of RAL. The objective of this study was to evaluate the safety and tolerability of RAL therapy and the rapidity with which RAL decreases viral load in HIV-infected pregnant women.
Methods: Women were considered for inclusion in the study if they were HIV-seropositive, =18 years of age, and received RAL during pregnancy. Men, non-pregnant women, or those that did not meet the inclusion criteria were not considered. HIV viral load, CD4 count (absolute), pregnancy demographics, antiretroviral regimens, adverse events, liver function enzymes, and APGAR scores were collected.
Results: Eight HIV-infected RAL-naïve pregnant women presented between 6 to 39.4 weeks gestational age with a median RNA viral load of 41,083 copies/mL at the initiation of RAL. From the initiation of RAL until delivery, the median decline in RNA viral load was 1.60 log. At delivery, two patients reached < 48 copies/mL and two had < 500 copies/mL. The median RNA viral load at delivery was 911 copies/mL. No adverse events in the mother or neonate due to RAL therapy were noted during this study.
Conclusions: This study suggests that RAL is safe and efficacious in HIV-infected pregnant women in the prevention of perinatal transmission of HIV. Further prospective study is needed.
Authors: Milena M McLaughlin, PharmD Midwestern University Chicago College of Pharmacy, Downers Grove, IL, USA Department of Pharmacy, Northwestern Memorial Hospital, Chicago, IL, USA *Audrey Galal, PharmD Department of Pharmacy, Northwestern Memorial Hospital, Chicago, IL, USA Jeannie Ong, BS, Midwestern University Chicago College of Pharmacy, Downers Grove, IL, USA Minh Dinh, MD Northwestern University, Division of Infectious Diseases, Chicago, IL, USA
ICHP Poster Presentations - Encore #2
Category: Encore
Title: Pharmacy consults on adult hospitalized patients with delirium
Purpose: To describe a unique pharmacy consult service and report provider acceptance on adult hospitalized patients having a positive assessment for delirium.
Methods: All adult patients over the age of 65 or exhibiting signs of altered mental status, admitted to a 616 bed, Level I trauma center, were assessed by nursing for altered mental status using a validated confusion assessment method (CAM) upon admission and at the change of shift. All positive CAM scores resulted in a consult to pharmacy to assess for possible drug causes. This report includes a retrospective chart review of these pharmacy consults from the beginning of the program in December 2012 to May 2014.
Results: There were a total of 1201 pharmacy consults, with a monthly average of 0.9 to 3.59 consults per day. The probability of drugs being the cause for the patients’ confusion was judged by pharmacists as unlikely, possible and definite. Positive CAM scores were attributed to opioids in 36.7% of consults and benzodiazepines were identified in 21.3%. The combination of medical, surgical and cardiac critical and intermediate care units comprised over 33.1% of the consults and 54% were from general care units. The level of acceptance was determined from 36 out of 224 consults randomly selected from the last 6 months of the study period. Pharmacists’ recommendations were accepted in 54.5% and 92.8% in which drugs were possibly or definitely associated with the patients’ confusion, respectively.
Conclusion: Pharmacist consults in hospitalized patients assessed to have delirium resulted in identification of a significant number associated with drug therapy, and the majority of pharmacists’ recommendations being accepted.
Authors: Ed C. Rainville*, MSPharm., Nikki P. Steenrod, MSN,CCRN, Tom E. Devlin, BSPharm., Michaela M. Doss, Pharm.D., BCPS, Cara L. Phillips Pharm.D., BCPS All authors are employed at OSF Saint Francis Medical Center, Peoria, Illinois
ICHP Poster Presentations - Encore #3
Category: Encore
Title: Outreach Program for Members of An ASHP Chapter
Purpose: Key to the success of any professional organization is its membership. An outreach program called the “Champion Program” was created to better connect with state chapter members and to offer additional member benefits. A member needs lists continuing education as a primary reason why members join. With decreasing resources for live local meetings, alternative methods for the delivery of continuing education needed to be established.
Methods: The state affiliate’s Marketing Affairs Division created the Champion Program to meet the needs of its current members. Previous need assessments had identified that members still wanted continuing education but in formats that made it easier for them to access, such as during the day or via home study. The Champion Program was designed to bring services directly to the member’s work place with a goal to identify a Champion at each Illinois hospital with an organization member. Marketing Affairs Division members contacted state chapter members at each member facility to request that they serve as a Champion. Champions were asked to post information provided to them concerning affiliate chapter activities and news, as well as coordinate live webinars organized through the affiliate chapter. Champions are sent an e-newsletter each month with affiliate chapter updates for them to either post or read during departmental meetings. Webinars are offered every other month on two separate dates for live continuing education and are also recorded for home study. Both members and non-members may take part in the webinars with CE credits provided free to members and a small fee for non-members. Only members may take advantage of the home study.
Results: By the end of the first year of the Champion Program, 48.4% of Illinois hospitals with at least one affiliate chapter member had an assigned Champion. This number has stayed relatively the same with 52.9% of member hospitals having a Champion by the end of 2013. Six webinar topics are provided each year with twelve live presentation dates which are then available as home study for two years. In 2013, 53.1% of member hospitals participated in at least one webinar presentation. On average, there are 6.25 hospitals participating in each webinar presentation. In 2013, only 15% of evaluations completed were for the home study format.
Conclusions: Members in areas of the state where no live continuing education programming is available through the chapter now have an opportunity to receive free continuing education. Though modest success has been seen with the program, there is still opportunity for greater volunteer involvement as well as continuing education participation. A Champion Program Task Force has been created to identify ways to improve the program. Potential actions include: creating a focused member needs assessment about the Champion Program; conducting a Champion focus group to identify perceived benefits or roadblocks; and establishing specific metrics to measure successes or opportunities for the program.
Authors: Patricia M. Wegner, BS Pharm, PharmD, FASHP* Vice President, Professional Services Illinois Council of Health-System Pharmacists Loves Park, IL; Jennifer Ellison, PharmD, BCPS Drug Information Pharmacist OSF St. Francis Medical Center Peoria, IL
ICHP Poster Presentations - Encore #4
Category: Encore
Title: Impact of PharmD clinic referrals on hemoglobin A1c in an outpatient clinic
Purpose: To assess the impact of PharmD clinic referrals on HbA1c levels in patients with diabetes within an outpatient clinic.
Methods: A list of patients with HbA1c >9% was evaluated for possible PharmD clinic referral. Pharmacist interventions from PharmD clinic referrals included adjusting medications, initiating new medications, counseling on lifestyle modifications, and addressing non-adherence to medications. HbA1c levels were compared from the start of the project and obtained at the end to track changes.
Results: This study included 59 patients with HbA1c >9% obtained from three PCP patient panels. Twenty-four patients were enrolled in the PharmD clinic. The average HbA1c improved from 10.2% (original list) to 9.2% (final list). For patients enrolled in the PharmD clinic, HbA1c improved to 8.5%. A new list was obtained at the end of the study incorporating new patients or patients previously<9%. This list showed a 19% decrease in the number of patients on three PCP panels with HbA1c >9%.
Conclusions: This proactive approach of targeting patients with HbA1c >9% decreased average HbA1c levels on each PCP team. There were some patients with HbA1c’s remaining >9% due to multiple other factors including non-adherence. However, the majority of patients decreased their HbA1c levels. This study demonstrates the positive impact an ambulatory care pharmacist can make through PharmD clinic referrals. Although the population was small, the results support pharmacists as integral members of the patient care team to improve outcomes for patients with diabetes in an outpatient clinic.
Authors: Diana Isaacs, PharmD, BCPS, BC-ADM, CDE* Clinical Assistant Professor Chicago State University Clinical Pharmacy Specialist-Ambulatory Care Oak Lawn VA Clinic (Hines VA) Dina Yousif, PharmD Candidate 2015 Chicago State University Lynn Huynh, PharmD Candidate 2015 Chicago State University
ICHP Poster Presentations - Student #1
Category: Student Research - Complete
Title: Adherence to IDSA guidelines for the treatment of Uncomplicated Cystitis in a Community Hospital Emergency Department
Purpose: To determine if improvement measures are warranted by evaluating adherence to the Infectious Disease Society of America (IDSA) guidelines for the antimicrobial treatment of urinary tract infections (UTIs) in an Emergency Department (ED), and evaluate susceptibility of organisms isolated from clean-catch urine samples to determine patterns of resistance to commonly prescribed antibiotics for UTIs.
Methods: A retrospective study was performed evaluating the cross-sectional data from electronic medical records (EMR) of otherwise healthy women aged 18-44 presenting to a community hospital ED with a primary diagnosis of UTI (599.0) over a period of 6 months. Adherence was evaluated based upon congruence with IDSA guidelines for appropriate antibiotic selection, dose, duration, and complete regimen. Additionally, the susceptibility results of isolates collected from clean-catch urine specimens from these same patients were used to determine antibiotic susceptibility. All results were analyzed using descriptive statistics.
Results: Adherence for the complete regimen was 14% for appropriate drug selection, dose, and duration for the 99 participants included in the study. Clean-catch urine cultures revealed 54% as mixed urogenital flora, thus no susceptibility results were performed. In cultures with a single organism isolated, Escherichia coli accounted for 88% of the cultures and was 78% susceptible to trimethoprim-sulfamethoxazole, 95% susceptible to nitrofurantoin, and 97% susceptible to ciprofloxacin.
Conclusions: Adherence to IDSA guidelines remains suboptimal, and despite this result ciprofloxacin resistance remains low. To prevent this resistance from increasing and to improve adherence, an opportunity exists to provide prescriber education and implement electronic medical record order sets.
Authors: *Kenneth William Gogol, BS, PharmD candidate at University of Illinois at Rockford; Kristi Stice, PharmD, BCPS, Pharmacy Clinical Coordinator, Kishwaukee Community Hospital
ICHP Poster Presentations - Student #2
Category: Student Research - Complete
Title: Staffing Requirements of PGY1 Pharmacy Residencies in Large Hospitals and PGY2 Pediatric Residencies
Purpose: Survey responses for post graduate year 1(PGY1) residencies in hospitals over 500 beds and all post graduate year 2 (PGY2) pediatric residencies as to their staffing requirements (hours worked and activities) and the person responsible for completing the performance evaluation for this staffing requirement were examined.
Methods: The survey was distributed electronically to 274 PGY1 programs and45 pediatric programs that were listed in the ASHP residency directory. Response rate for PGY1 residencies was 44% and 62.2% for PGY2 pediatric residencies.
Results: Average hours spent staffing were usually scheduled on a weekend and averaged approximately 30 hours a month for PGY1 residencies and approximately 26 hours a month for PGY2 residencies. The most common staffing activities performed by the residents included order verification and supervision of technicians/support staff. Other staffing activities included pharmacokinetic consults, automated drug cabinet checking, intravenous admixture compounding, and patient education. The performance evaluation for the resident’s staffing requirement was most commonly completed by either the operation manager or the residency director on a quarterly basis for both for PGY1 and PGY2 residencies. Assigned preceptors and the charge pharmacist were also mentioned as completing the evaluation for a large portion of residencies responding.
Conclusion: Staffing requirements for a resident averaged about 30 hours per month, mostly on the weekends. The staffing activities performed by the resident varied depending on the program. A performance evaluation for the resident’s staffing duties was usually completed by the operations manager on a quarterly basis.
Authors: Cody Lloyd Schaefer*, PharmD candidate, Southern Illinois University Edwardsville Jennifer C Ellison, PharmD, BCPS, PGY1 Residency Program Director, Drug Information Pharmacist, OSF St. Francis Medical Center Julie L Kasap, PharmD, Children's Hospital of Illinois Pharmacy Supervisor, OSF St. Francis Medical Center
ICHP Poster Presentations - Student #3
Category: Student Research - Complete
Title: The Forgotten Transition of Care: Discharge Protocol from Hospital to Community Pharmacy
Purpose: The purpose of this study was to create, implement, and evaluate the results from a discharge protocol between a hospital and community pharmacy.
Methods: In this single-center study, patients admitted to the study hospital who were ages 18 years and older and used the designated community pharmacy were used in the research. Upon discharge from the hospital, the hospital sent the patients’ discharge medication lists to the community pharmacy. The study tracked measures used by the Centers for Medicare & Medicaid Services (CMS) and the Pharmacy Quality Alliance (PQA), such as discontinued oral diabetes medications, ACE inhibitors or ARBs, and high-risk medications in the elderly. It also evaluated discrepancies between the patients’ hospital and community pharmacy medication profiles.
Results: There were 51 patients included in this month-long study. The majority of the study population was females age 65 years and older. None of the discontinued medications were oral diabetes medications, ACE inhibitors, or ARBs. Almost 8% of patients were instructed to stop using a high-risk medication. Approximately 41% of patients had home medications stopped at discharge. Over half of the patients’ medication profiles showed discrepancies between the hospital and community pharmacy.
Conclusions: This study demonstrated discrepancies between hospital and community pharmacy profiles. The discharge protocol can help community pharmacies and health plans improve performance as measured by the CMS and PQA by informing the community pharmacies of patients’ discontinued medications that they would not otherwise know.
Authors: Megan Ashley LeBaron*, PharmD Candidate, Southern Illinois University Edwardsville School of Pharmacy Kristi Stice, PharmD, BCPS, Kishwaukee Hospital
ICHP Poster Presentations - Student #4
Category: Student Research - Complete
Title: A Business Plan to Enhance Access to Quality Care among Veterans in Rural Communities
Purpose: A need assessment and SWOT analyses were conducted to develop a business plan for improving access to care among veterans in rural areas in IL and MO.
Methods: Literature review, a need assessment, and SWOT analyses were conducted by a pharmacy faculty and student pharmacists to identify areas in Illinois and Missouri that do not provide adequate care to veterans. A business plan was developed to provide a Mobile Medical Unit (MMU) that will enable pharmacists and student pharmacists to conduct health screenings, offer preventive medicine, and provide ambulatory care for members of the US Armed Forces, Veterans, and their families.
Results: Results of the market analysis showed that in approximately the last decade, the rural Veteran population accounts for 40 percent of all VA patients. Between 1997 and 2001, five million US Veterans, used a VA acute care hospital and/or outpatient clinic. Currently there are approximately 1.3 million Veterans who reside in Illinois and Missouri. SWOT analyses showed that MMU will improve access to care for veterans who are in debilitating conditions, lack transportation, and cannot afford to travel long distance to VA clinics.
Conclusions: Given the unmet needs of veterans in rural areas in Illinois and Missouri, pharmacists and student pharmacists are poised to meet these needs. Recent reports of lack of access to care, having mobile medical units may alleviate the burden of illness among the veterans and enhance access to quality and timely care among veterans in local and national rural areas.
Authors: Blaine A. Johnson1, PharmD Candidate***; Joseph S. Morgan1, PharmD Candidate; Dahlia Uwimbabazi1, PharmD Candidate; Abby A. Kahaleh2, BPharm, MS, PhD, MPH*;
1,2Roosevelt University College of Pharmacy
ICHP Poster Presentations - Student #5
Category: Student Research – In Progress
Learning Objective: To identify methods used by Illinois postgraduate training programs to educate trainees on how to perform a quality peer review.
Title: Peer Review Opportunities and Training in Illinois Residency and Fellowship Programs
Purpose: Journals often utilize a peer review process to determine acceptability of submitted manuscripts for publication. For most journals, there is no formalized training or certification to become a peer reviewer, and often journals struggle finding quality reviewers. Focusing on educating trainees earlier on in their career may have a greater and more sustained impact on their ability to provide a quality review. Currently, there is no published study that has specifically evaluated what type of training is provided to residents, fellows and/or students on the peer review process. The purpose of this project is to identify what strategies are currently used in Illinois pharmacy residency and fellowship programs to educate residents, fellows, or pharmacy students on how to perform a quality peer review. A survey will be distributed in January 2015 to all residency and fellowship directors in the state of Illinois in the form of an electronic questionnaire built in SurveyMonkey. In addition to demographic information, the survey questions will ask if a peer review is required, how many peer reviews are performed, whether another faculty/practitioner assists the resident in performing the review, and what methods are used to educate the trainee on the best way to conduct a peer review.
Authors: Rebecca Myers, B.S. * Student Pharmacist, Class of 2016 Midwestern University Chicago College of Pharmacy Jen Phillips, PharmD, BCPS* Assistant Professor, Pharmacy Practice Midwestern University Chicago College of Pharmacy Robin Zavod, PhD Associate Professor of Pharmaceutical Sciences Midwestern University Chicago College of Pharmacy
ICHP Poster Presentations - Student #6
Category: Student Research – In Progress
Title: Hedgehog and Tyrosine Kinase Inhibitors for Treating Breast Cancer
Purpose: Majority of breast cancer patients relapse and progress to metastatic disease despite initial response to chemotherapy. The reasons for chemoresistance include presence of cancer stem cell (CSC) sub-populations possessing tumorigenic potential and upregulated oncogenic pathways. Therefore, the objective of this study was to investigate the anti-proliferative effects of two tyrosine kinase inhibitors (afatinib and gefitinib) and two hedgehog inhibitors (vismodegib and cyclopamine) to identify potential synergistic combinations for treating breast cancer. The effect of afatinib, gefitinib, cyclopamine and vismodegib on the growth of breast cancer cells in vitro was first examined. Using a combination of MTT assay, isobologram analysis and response surface modeling, combination of afatinib or gefitinib with vismodegib or cyclopamine was observed to be synergistic in their ability to inhibit breast cancer cell growth. This effect was found to be dose, time, cell line and schedule dependent. Also, since the anticancer agents studied are extremely hydrophobic, polymeric micelles were fabricated using lactic acid and carbonate based copolymers to improve drug solubility. Polymeric micelle formulations were found to increase the aqueous solubility of these compounds several fold.
Authors: Elvis Boamah, PharmD student,Chicago State University College of Pharmacy Qudus Ibrahim, PharmD student,Chicago State University College of Pharmacy Ruchi Patel, PharmD student,Chicago State University College of Pharmacy Dolapo Ajayi,PharmD student,Chicago State University College of Pharmacy Michael Danquah, [Faculty] PhD, Chicago State University College of Pharmacy
ICHP Poster Presentations - Student #7
Category: Student Research – In Progress
Title: A retrospective chart review of chronic pain medication management
Purpose: Chronic pain characteristics and appropriate treatment vary greatly from patient to patient. Medications for chronic pain are titrated and changed for patients to maximize pain relief. It is unclear how changes such as deciding to increase the dose or change to a different medication are made. The purpose of this study is to determine how chronic pain medications have been managed for patients within the Southern Illinois University (SIU) Healthcare system in Springfield, Illinois.
Methods: Retrospective chart review was completed for approximately ten consenting patients in a related prospective cohort study which aimed to educate patients on various topics relating to chronic pain. Eligible patients are 18-89 years old who are active patients within the SIU Healthcare system and diagnosed with chronic, non-cancer pain. Data collected includes patient demographics, pain diagnosis, pharmacologic and non-pharmacologic treatments for pain, duration and reason for treatment changes, and whether or not medication changes occurred after attending the first education session provided by the parent study.
Results: In progress – will be available by poster session
Authors: Lauren Nicole Kormelink* Pharm.D candidate, Southern Illinois University School of Pharmacy Carrie Vogler Pharm.D, BCPS, Clinical Assistant Professor at Southern Illinois University Edwardsville School of Pharmacy
Leadership Profile
Noelle Chapman, PharmD
 Where did you go to pharmacy school?
Where did you go to pharmacy school? University of Wisconsin—Go Badgers!
Trace your professional history since graduation. Where have you trained or worked? Any special accomplishments?
After graduating from pharmacy school, I completed a Pharmacy Practice Residency at Northwestern Memorial Hospital (NMH). After completing my residency, I stayed on at NMH and worked with cardiology/critical care patients for a short time before moving to the Anticoagulation Dosing Service where I stayed for almost 4 years. While working in anticoagulation, we were able to complete a quality improvement project that examined pharmacist dosing of heparin. This project led to the expansion of our critical care services, the development of our medicine team and other clinical service lines, and it fueled my passion for service development and experiential education. In 2007, I had the opportunity to take a leadership position in clinical operations, and there was no looking back! I have been blessed to be able to blend clinical services with operations management, as well as leadership development, in my role as pharmacy manager. Additionally, I am the PGY1 Residency Program Director, which continues to fuel my enthusiasm for developing practitioners who challenge the status quo.
What initially motivated you to get involved, and what benefits do you see in being active in a professional association such as ICHP?
My initial motivation to get involved in ICHP really stemmed from my curiosity for new opportunities. I was approached to do a residency roundtable at the ICHP Annual Meeting a few years back, and I had so much fun and learned so much from the people I met that I was hooked. I feel there is a lot of value in being active in professional organizations. Learning from others who are facing similar issues, networking, generating new ideas, professional development, giving back – the list goes on and on.
What advice would you give to a new practitioner eager to become more involved within ICHP? To the new graduate? To the student?
Don’t be afraid to try something that you may be unfamiliar with and do not be passive with your experiences. Often your experiences will lead you to another opportunity until you find a fit for your passions, but that only happens if you are actively seeking it. I think it is relatively easy to get involved when you are a student; however, establishing that habit when you have graduated can be difficult. Find a mentor, if you don’t know where you fit. Once you are involved, remember how you felt and don’t be afraid to reach out to others.
Is there an individual you admire or look up to, or a mentor that has influenced your career?
There are so many people! I truly want to learn something from everyone I encounter. Some of the people that I admire include:
My husband teaches me to stay focused on what is really important, yet, relaxed in my approach
My parents teach me generosity and how to work hard and effectively
My kids teach me something new every day. I love seeing the world through their eyes!
Some of my professional mentors include:
Desi Kotis—Desi is a huge mentor to me. She emulates how to not be afraid to have big thoughts and push boundaries and is extremely supportive of my personal journey.
Mike Postelnick—Mike Postelnick constantly reminds me the value of teamwork and reaching for the stars.
Mike Powell (UNMC)—Mike Powell really cares about people as people and always has time to give terrific advice.
Steve Rough (UW)—Steve is not afraid to take the world by storm and inspires me to do the same.
As a newer practitioner, what is your vision for Pharmacy in the future? Or what would you like to able to see accomplished within Pharmacy?
First, thanks for calling me a newer practitioner? Second, I would love to see patients demand that a pharmacist be involved in all levels of their care. In order to accomplish this, we need to pull together as a profession across various care settings to prove our worth to individual patient and public health.
What three adjectives would people use to best describe you?
I ask this question to the PGY1 residents about themselves every year so my words have been well vetted with those close to me: enthusiastic, reasonable, insightful.
Do you have any special interests or hobbies outside of pharmacy/work/school?
I love to read, but I read actual books (versus on an e-reader) because I’m building a library in which I only put books that I’ve read. I recently found out I’m creative! I like to make crafty gifts and build things. Also, I am the ultimate soccer mom. Three of my four children play on two teams each year round, and my husband coaches five of those teams. The fourth child doesn’t play yet because she was only born in October, BUT she did get a soccer ball for Christmas!
Do you have a favorite restaurant/food?
Cheese. Hands down. I am a Wisco girl after all.
What is the most interesting/unique fact about yourself that few people know?
I am a nut for college basketball, particularly the NCAA tournament.
ICHPeople
Congratulations to ICHP members, Noelle Chapman, Ann Jankiewicz, and Chris Qullian, on being named ASHP Fellows for 2015!
The ASHP Practitioner Recognition Program is intended to recognize excellence in pharmacy practice and promote public awareness of pharmacists who have distinguished themselves in practice. Please congratulate the ASHP Fellows for 2015. They will be honored on Tuesday, June 9, 2015, during the ASHP Summer Meeting in Denver, Colorado.
- See more about ASHP Fellows at: http://www.ashp.org/ashpfellows#sthash.pj3L5129.dpuf
Congratulations to the Platform Presenters and Poster Winners from the ICHP/MSHP 2015 Spring Meeting!Michael Santini - Winner - Platform Presenter
Bryan McCarthy - Platform Presenter
Kushal Shah - Original Winner
Ed Rainville - Encore Winner
Blaine Johnson - Student Winner
Megan LeBaron - Student Winner
Congratulations to Bernice Man who was selected as one of twelve winners of ASHP's Campus and Practice Leadership Award!
About the Award
ASHP has recognized twelve pharmacy students for their achievements in campus leadership and pharmacy practice in hospitals or ambulatory care clinics (including professional work experience, internships, and other accomplishments) with the ASHP Student Leadership Award.
The award, sponsored by ASHP and the ASHP Research and Education Foundation, is given to student members in their second through fourth professional years of pharmacy school. The award winners receive a plaque, an ASHP drug information reference library, and a $2,000 cash award.
Government Affairs Report
The Bills Are Here!
by Jim Owen and Scott Meyers
It didn’t take the 99th Illinois General Assembly long to introduce 6318 bills between January 14th and February 27th! ICHP is monitoring 82 of those bills that may or may not have an impact on Pharmacy. Here’s a summary of the bills that are out there, in the order of current importance to ICHP.
HB0001 The Heroin Crisis Act – This single bill amends 24 existing Illinois Acts and has some very onerous language for pharmacies. The bill requires all pharmacies to establish medication take-back programs that include controlled substances, but it does not provide for payment of the implementation or ongoing reverse distributor costs associated with such a program. The take-back receptacles will need to be placed where pharmacy personnel can observe them at all times but pharmacy personnel are not allowed to place any returned medications in the receptacle. These receptacles will take up valuable retail or patient waiting area space, will add to security concerns for the pharmacy with additional risk of burglary or robbery and additional costs to the pharmacy related to increased insurance payments as a result of the risks. The bill also virtually requires the pharmacy to check the Prescription Monitoring Program (PMP) for every controlled substance prescription while leaving the prescriber without a similar responsibility. HB1 also creates a confusing limitation on the day supply of CII medications allowed to be prescribed or dispensed. The prescriber is limited to writing an initial 10-day supply with up to two additional sequential prescriptions for the same. However, if the prescriber is familiar with the patient and confident that no abuse or resale of the controlled substance will occur, he or she may prescribe up to three 30-day supplies of the controlled substance. The Act does contain several redeeming qualities such as expanded public access to naloxone, establishment of drug courts and a tightening of the PMP. ICHP is working with IPhA and IRMA to provide some alternative language for the problems with this bill in order to take a step forward in the fight against heroin and opioid addiction.
SB1611 and HB3519 Biosimilars – Both of these bills would require pharmacists to notify a prescriber when an interchangeable biosimilar is interchanged with a product ordered by the prescriber. The Senate bill requires prescriber notification in a “reasonable time” while the House bill calls for notification within 72 hours. Currently the FDA Purple Book states “An interchangeable biological product is biosimilar to an FDA-approved reference product and meets additional standards for interchangeability. An interchangeable biological product may be substituted for the reference product by a pharmacist without the intervention of the health care provider who prescribed the reference product.” Both Illinois initiatives would restrict the access to and interchange of less expensive biosimilars, increasing the costs of medications and confusing patients on the safety and efficacy of the medications their prescription medication provider (insurance, Medicare or Medicaid) requires them to receive. ICHP is working with the sponsors of both bills to prevent passage of any language more stringent than that of the FDA.
HB3271 Certified Pharmacy Technician CE – Sponsored by Rep. Michael Zalewski of Riverside, the bill would amend the pharmacy practice act to require that all certified pharmacy technicians are required to complete 20 hours of continuing pharmacy technician education every two years including one hour of law and one hour of patient safety related CE. The amendment would also move certified pharmacy technicians to a two-year renewal on the opposite year as pharmacists and pharmacies. This would even out the workflow and cash flow for the Department of Financial and Professional Regulation. Registered technicians and student pharmacists would continue to renew annually. ICHP supports this bill.
HB3627 Expanded Access to Immunizations – Sponsored by Rep. Marcus Evans Jr. from Chicago, this bill would expand the pharmacist’s ability to provide patients age 10-13 with all types of immunizations. Currently, pharmacists may only immunize this specific population for seasonal influenza and TDaP. The bill amends the Pharmacy Practice Act and is strongly supported by ICHP, IPhA and IRMA. There is currently strong opposition from pediatricians and county health departments.
HB0421 Amends the Nurse Practice Act – Rep. Sara Feigenholtz has sponsored this change which would eliminate the requirement for written collaborative agreements between physicians and advanced practice nurses. ICHP is strongly opposed to this bill as it will be very difficult for any pharmacy to determine if an APN has prescriptive authority for the prescriptions they write.
SB0029, HB0207, HB0496, HB1335 and HB2508 The Right To Try – These five very similar bills would allow patients, who have been diagnosed by their physician as terminally ill, to petition pharmaceutical manufacturers to obtain investigational medications that have completed Phase I trials and that may provide relief for their condition. These bills provide limited liability protection for the physician involved, they do not mandate that the manufacturer must provide the drug or provide the drug free of charge. The problem is that these bills circumvent the current FDA policy on Compassionate Use and provide no real safety for the patients who may seek to use these medications. ICHP is opposed to these bills for those reasons.
HB3774 Notification of the patient prior to shipping meds – Rep. Monique Davis of Chicago would like to amend the Pharmacy Practice Act requiring all pharmacies and non-resident pharmacies to notify the patient in advance of shipping medication so as to allow them the opportunity to decline the shipment. ICHP is currently neutral on this bill.
A variety of bills amend the Public Aid Code – Most bills either ask to remove the four prescription prior authorization limit or exempt drug classes from the prior authorization requirement. Medications such as oncolytics, anti-retrovirals, immunosuppressants, anti-depressants, anti-psychotics, anti-anxiety and smoking cessation products would be exempted by one or more bills. In addition, one bill would reestablish the ability of a prescriber to right a prescription for an OTC medication to be filled in a pharmacy in the same manner and reimbursement as prescription medications. All of these bills would reverse much of the savings obtained by the SMART Act in 2012. ICHP is currently neutral on these bills.
A variety of Opioid Abuse Prevention Bills – In addition to HB0001, there are several House and Senate bills that are aimed at opioid abuse prevention. Most will be rolled into the comprehensive HB0001; however, there are several bills that would restrict the use of non-abuse deterrent opioid analgesics for any patient with prescription drug coverage including Medicaid. These bills are unlikely to move forward in any form. There are two other bills that would require pharmacies to dispense CII opioid analgesics in a special single use locking vial that would increase the costs of prescriptions significantly without any real deterrent for diversion. These too will hopefully fail this session.
The initial deadline for bills to be passed out of their respective committees is March 27th, which will have passed by the time of this publication. There are always bills that can have their deadline extended, and we assume that may happen this year with some of the legislation we are watching. We may reach out to you, our members in the next 2-3 months to call, email or visit your legislators on one or more of these issues. We hope this session is positively productive for our patients and our profession, and we will work diligently with the members of the General Assembly to see that it happens.
Board of Pharmacy Update
Highlights from the March Meeting
by Scott A. Meyers, Executive Vice President
The March 10th Board of Pharmacy Meeting was held at the James R. Thompson Center at Randolph and LaSalle Streets in Chicago. These are the highlights of that meeting.
New Board Member – The Board members welcomed new Board Member Rick Mazzotti from Taylorville. Rick was appointed to the Board by former Gov. Quinn in January. His pharmacy background is in community pharmacy and he spent several years working for the State of Illinois in the Medicaid division.
Rules Update – Daniel Kelber, general counsel for the Board announced that the Joint Committee on Administrative Rules (JCAR) had accepted the proposed Controlled Substance Act Rules, and they will be published in the March 13th Illinois Register. The Rules' changes effect several areas of the Act, and an overview will appear in the next issue of KeePosted. The public comments on the first draft of the Pharmacy Practice Act Rules are still being reviewed and responses are being written. It is expected that a final draft of these rules will go to JCAR sometime in late April. The Department must first collate all the suggestions and written responses to each comment received and return those to the commenters. Then they will be sent to JCAR for final review. It is hoped that these rules will be in place by the end of the year. Students graduating this spring will not be tested on any of the new rules but may see some test questions that are being evaluated that could relate to the new Controlled Substance Act Rules. These test items will not count toward the graduate’s actual score.
Future Meetings of the Board – The Board drafted a tentative schedule for its meetings during the 2016 Fiscal Year. Here are the tentative dates and locations:
July 14, 2015 Chicago
September 15, 2015 Chicago
November 10, 2015 Chicago
January 12, 2016 Chicago
March 8, 2016 Springfield
May 10, 2016 Chicago
NABP Annual Meeting – This year’s Annual Meeting of the National Association of Boards of Pharmacy (NABP) will be held on May 16-19, 2015 in New Orleans, LA. Several members indicated that they would attend. Members who attend do so at their own expense.
2015 NABP District IV Meeting – The District IV meeting, which is a joint meeting with the American Association of Colleges of Pharmacy, will be held on November 4-6 in Milwaukee, WI. It will be jointly sponsored by the Wisconsin Board of Pharmacy and Concordia University, College of Pharmacy.
2016 NABP District IV Meeting – The 2016 District IV meeting is scheduled to be cohosted by the Illinois Board of Pharmacy and the University of Illinois at Chicago. Dean Bauman of UIC had contacted Board Member, Phil Burgess asking if the meeting could be held in Rockford in order to showcase the new Rockford Campus. The Board did not agree and will recommend to NABP that the meeting be held in the downtown Chicago area. Board members felt that attendees from other states come to this meeting to see and enjoy the offerings of downtown Chicago. They discouraged using any site like Rosemont which would also be several miles from most attractions. NABP will decide the final location.
MPJE Item Writing – The Board will be writing new test questions (items) for the Multi-State Jurisprudence Examination in March and asked the Department staff if proposed rule changes could be included. Approved changes to the Controlled Substance Act may be included but proposed changes to the Pharmacy Practice Act may not as there is no guarantee that they will be approved. New test questions will be tested for several months to ensure that they are psychometrically sound and legally defensible before they may be included in the scored portion of the test, so candidates taking the MPJE for Illinois in the next six months or so should focus on current Pharmacy Practice Act, Controlled Substance Act and respective rules.
Legislative Update – The March legislative update was presented by Scott Meyers, ICHP Executive Vice President. There are a significant number of bills impacting pharmacy this legislative session and a summary of those bills appear in this edition of KeePosted in the Government Affairs Report.
Visitor Comments – Doug Higgins, pharmacist and owner of Doug’s Compounding Pharmacy in Paxton, IL reported to the Board that the FDA has now published a revised list of drugs that may be compounded that are not FDA approved or found in the USP-NF and also a revised list of drugs that should not be used in compounding. Two of the drugs that should not be compounded are bevacizumab (Avastin®) and any non-abuse deterrent hydrocodone product. He also expressed concerns about recent regulations related to the Drug Supply Chain Security Act that require Memorandums of Understanding between the FDA and States in order to allow expanded interstate delivery of compounded products. He also emphasized concerns about the proposed USP Chapter 800 that is currently in second draft form. It appears that this USP chapter is extremely prescriptive and will cost every pharmacy significant expense in renovation in order to become compliant in handling hazardous materials (medications) within the pharmacy.
Next Board of Pharmacy Meeting – The next meeting of the Illinois Board of Pharmacy will be held at 10:30 AM on Tuesday, May 12th at the James R. Thompson Center in Chicago. The profession is welcome to attend the open portion of this meeting.
Medication Safety Pearl
Use of a Technician Double Check System to Help Reduce IV Compounding Errors
by Geri Anderson, MHA, CPhT, Pharmacy Technical Services Manager (1) and Jen Phillips, PharmD, BCPS, Clinical Specialist Drug Information (1) and Assistant Professor (2)
1Lutheran General Hospital 2Midwestern University Chicago College of Pharmacy
INTRODUCTION
There are many published studies that have evaluated the accuracy of a technician double-check process for unit dose medications.1-6 Use of a technician double-check system has resulted in a decrease in the reported numbers of dispensing errors with a cart fill system at some institutions. Data suggests that pharmacy technicians can perform this task as accurately or sometimes more accurately2,5 than pharmacists, and some states allow “tech-check-tech” programs for refilling of unit dose medication dispensing systems.7 A pilot tech-check-tech project performed in California found that technicians had a mean accuracy rate of 99.89% compared to 99.52% for pharmacists (p<0.0001).2
There is less data assessing technician accuracy in checking intravenous (IV) preparations. One study compared the accuracy rates of pharmacists and technicians when checking IV syringes for a dialysis program. No differences in the accuracy rate were found between pharmacists and technicians (99.86% vs. 99.83%, respectively). There is no data on how the use of a technician double-check in addition to a pharmacist check may further reduce the number of errors. The purpose of this project was to determine if a technician double-check, in addition to a pharmacist check, could reduce the number of IV compounding errors at a large, community teaching hospital.
Advocate Lutheran General Hospital (ALGH) is a 638-bed hospital serving Chicagoland’s northern suburbs. It is a community teaching hospital and a level one trauma center. ALGH employs 56 pharmacists and 51 technicians. ALGH prepares an average of 642 IV products daily. Approximately 169 (26%) are compounded products.
PROCESS
In May of 2014, a technician double-check process was implemented for all IV batched products compounded in the IV room. Prior to compounding the IV product, the chemo technician sorts the batch according to drug/concentration and selects the correct product(s) for compounding, including additive and base fluids, and places each label with products on a separate tray. The batch technician double-checks that all products selected are correct and initials labels in lower corner indicating approval to compound the product. The IV batch is still checked by a pharmacist after compounding and prior to the IV being sent to the floor. The addition of a technician double-check adds approximately an extra ten minutes every time the batch is prepared and there are four batches prepared per day.
To evaluate the effectiveness of this additional safety check, the Department of Pharmacy tracked the number of compounding errors reported prior to and after implementation of the new process. From January to March 2014, a total of 9,488 doses were compounded and 60 errors were reported by the pharmacist prior to delivery to nursing unit, for an event-rate of 0.006, or about 1 error per 166 doses compounded. From July to September of 2014, a total of 21,336 doses were compounded and a total of 22 errors were reported, for an event-rate of 0.001, or about 1 error per 1000 doses compounded. Thus, use of a technician double-check prior to compounding resulted in an 83% reduction in the compounding error rate. (p<0.0001).
LESSONS LEARNED
When this process was first implemented, it took some time to get the technicians acclimated to the new process. To help alleviate this, reminders were provided via email and during staff meetings. In addition, the technician manager would stop by during the time of the IV batch compounding to help remind the technicians. Over time, this process has become more “hard-wired” in the technician workflow. Once errors are identified, the technician who compounded the product is the one to correct the error. Lessons learned were to be able to correct a co-worker as well as being able to receive constructive criticism from a peer. No punitive action is taken, and any opportunity to identify process improvements is welcome.
FUTURE INITIATIVES
Future initiatives include expanding this process to include not just compounded products, but also premade products that are labeled in batches. It is anticipated that use of a double-check process in this area will help further reduce the number of dispensing errors. The Department will continue to track the impact of this process on error rates.
Figure 1: Compounding Error Rates: January to September 2014
CONCLUSION
An independent double-check is a process in which two technicians separately check all components of a compounded product for accuracy before the compounding begins. These independent double checks have led to a reduction in pharmacist reported errors while adding minimal (less than 15 minutes) to the workflow of the technicians.
REFERENCES
- Reed M, Thomley S, Ludwig B, Rough S. Experience with a “tech-check-tech” program in an academic medical center. Am J Health-Syst Pharm. 2011;68:1820-3.
- Ambrose P, Saya E, Lovett L, et al. Evaluating the accuracy of technicians and pharmacists in checking unit dose medication cassettes. Am J Health-Syst Pharm. 2002;59:1183-8.
- Spooner SH, Emerson PK. Using hospital pharmacy technicians to check unit dose carts. Hosp Pharm. 1994;29:433-7.
- Anderson S, St Peter J, Macres M, et al. Accuracy of technicians versus pharmacists in checking syringes prepared for a dialysis program. Am J Health-Syst Pharm. 1997;54:1611-3.
- Ness JE, Sullivan JD, Stergachis A. Accuracy of technicians and pharmacists in identifying dispensing errors. Am J Health-Syst Pharm. 1994;51:354-7.
- Woller T, Stuart J, Vrabel R, et al. Checking of unit dose cassettes by pharmacy technician. Am J Hosp Pharm. 1991;48:1952-6.
- Adams AJ, Martin SJ, Stolpe SF. “Tech-check-tech”: A review of the evidence on its safety and benefits. Am J Health-Syst Pharm. 2011;68:1824-33.
College Connections
Ronald McDonald House
by Saba Hamid, P2, ICHP Historian, Midwestern University Chicago College of Pharmacy
On Saturday, January 24, the student chapter of ICHP from Midwestern University volunteered at the Ronald McDonald house near Loyola Medical Center and Hines VA Hospital. We went to the house to cook a meal for the families staying there. These families have children who are pediatric inpatients in the hospital. At the end of the day, when the families finished visiting their son or daughter for the day, they could come back to the house where they could eat a meal cooked by a group of volunteers. With our group of 7, we served pasta with mixed vegetables on the side and brought pink lemonade and cookies to share with the people who were staying there. In all, we were able to serve to about 5 people, but we understood that more would come at a later time when visiting hours were over. After 4 hours of cooking, serving and cleaning, we left a note to the guests that they could help themselves to the food we cooked since it was meant serve 30 people.
Afterward, we went on a tour of the house, since this was our first time there. The house has several rooms where parents can stay while their children are going through treatments. The Ronald McDonald house is a non-profit organization that provides comfort to all parents whose children are hospitalized around the Chicagoland area and is conveniently located near hospitals.
Volunteering was a good way to take some time off from studying for exams and do something to take our minds off it. Our philanthropy chair, Chau Tran, who organized this event shared, “Although we did not serve as many people as we would have liked, knowing that we did something to help ease the transition for the parents and families gives us a great sense of accomplishment. Oftentimes, in times of sadness and hardship, no one wants to take on tasks that are time-consuming and trivial such as cooking. I felt that we helped ease the stress on the families because they did not have to worry about finding a meal for that day. This is something I hope we can continue to provide in the future because even though we are constantly busy and working hard towards becoming pharmacists, volunteering is still something that everyone should do, whether it is a regular thing or not.” Reaching out to the community and doing something good made us feel glad to have organized and done this activity.
Knowing the Potential of Our Future Career
by Gary Chu, P3, ICHP-SSHP Philanthropy Chair, Rosalind Franklin University of Medicine and Science, College of Pharmacy
While in school, our minds are occupied with a large amount of schoolwork; our focus is on the didactic aspects of the basic sciences and developing clinical knowledge. However, in the real world, being academically strong is only half of the equation. Skills such as communication, adaptability and being a team player complete the success equation. For example, a pharmacist must know how to communicate effectively and professionally in order to participate on an inter-professional team caring for a patient and counsel and educate a patient on their medications.
The RFUMS ICHP-SSHP chapter introduced me to a volunteer opportunity at a hospice service company during the beginning of my 2nd professional year. I wanted to make a difference and was attracted to this great opportunity. This opportunity is at the V Care Hospice located in Northbrook, IL. V Care Hospice is an inter-professional team of nurses, chaplains and social workers assisting patients as they walk the final steps of their life’s journey. This service is very meaningful to the patient and their family and made me recognize the importance of palliative and hospice care.
At school, we focus on treatments and cures for diseases and how to monitor for efficacy and safety using objective parameters like blood glucose, INRs and blood pressures. Hospice care services focus on comfort, pain relief and the overall dignity of the patient as they approach the end of life. This volunteer experience has given me a completely different point of view on the care of a patient. Pharmacists can contribute significantly to the care of a patient at the end of life. The contribution could be as simple as recommending a comfort chair that helps patients stay comfortable when immobilized or as complex as developing an optimal medication regimen that minimizes adverse reactions and drug interactions. In addition, pharmacists need to recognize and recommend the dosing of opiate medications, which are often much greater than normal, and other analgesic products in order to provide comfort for patients.
I would like to thank our e-board members from the first pharmacy class at RFUMS COP for giving us this chance to increase our knowledge while expanding the diversity of professional pharmacy practice. I am proud to be an ICHP–SSHP member and an e-board member of Rosalind Franklin University of Medicine and Science. I plan to encourage further volunteer opportunities for our members during my time in pharmacy school.
Legislative Day
by Julia Sapozhnikov, University of Illinois College of Pharmacy Pharmacy Student, Class of 2017
 On Wednesday, March 11, 2015, ICHP and IPhA held the 9th Annual Illinois Legislative Day in Springfield, IL. This tradition has been a great opportunity for the profession of pharmacy to unite together in the State Capitol and have our voice and ideas heard.
On Wednesday, March 11, 2015, ICHP and IPhA held the 9th Annual Illinois Legislative Day in Springfield, IL. This tradition has been a great opportunity for the profession of pharmacy to unite together in the State Capitol and have our voice and ideas heard.
Upon arrival, students from pharmacy schools all over the Chicagoland area and the Midwest gathered in the Auditorium. It was a great opportunity to network with students from other areas and listen to their opinions about current events in pharmacy. We were honored to have the Lt. Governor Evelyn Sanguinetti and Representative Michael Zalewski welcome us to Springfield. They both thanked the profession of pharmacy for our hard work, integrity, and the care we have for our patients. After these acknowledgments, an older gentleman who has owned his own pharmacy for 42 years spoke passionately about how many important services pharmacists provide and how they should get paid for what they do. Specifically, he voiced his concerns about the long amount of time it takes for Medicaid to reimburse independent pharmacies and how much that has affected him.
Next, Scott Meyers, the ICHP Executive Director, and Garth Reynolds, the IPhA Executive Director, presented some of the key bills being debated in Springfield at the moment. Specifically, they focused on a few key bills that may have a big impact on pharmacy and that they wanted us to focus on when we went to speak to our individual legislators. Senate Bill (SB) 1611 requires mandatory medication take back by pharmacies. There are several concerns about this bill including the cost of maintaining the disposal program as well as the increased safety concerns of holding controlled substances at pharmacies, especially because pharmacies are already targets for armed robberies. We recommended the continuation of medication take-back programs at law enforcement facilities because they are already established and are better equipped to deal with the safety concerns. The other part of the bill addressed how to limit Schedule II controlled substances to a 10-day supply per prescription. IPhA and ICHP also opposed this bill because of the cost as well as the inconvenience of placing excessive barriers to obtain C-II prescriptions, such as ADHD medications for children. A few bills that pharmacy supported were HB3271, which addressed continuing education for pharmacy technicians, and HB3627, which addressed expanded immunization capability for pharmacists.
After the information session, crowds of pharmacists and students in white coats headed down the streets of Springfield toward the Capitol building. Divided in groups, we each went to the offices of our Representatives or Senators to speak to them about these key bills. It was great to hear the legislator’s input on certain issues and to see how well they listened and were interested in what we had to say. They were excited to have young adults visit them.
To end the day, we all gathered on the staircase outside of the Capitol Building for a group photo with The Honorable Governor Bruce Rauner. It was a great privilege to be acknowledged and thanked by our Governor. As we sat in our bus seats getting ready for the 3 hour ride back to Chicago, we all had great thoughts from the day and were excited about everything we learned and the comradery we felt while united together as a profession.
More
Officers and Board of Directors
LINDA FRED
President
GINGER ERTEL
Treasurer
660-342-5022
gertel@msn.com
CHARLENE HOPE
Secretary
708-783-5933
TRAVIS HUNERDOSSE
Director, Educational Affairs
thunerdo@nmh.org
CARRIE VOGLER
Director, Marketing Affairs
217-545-5394
DESI KOTIS
Director, Professional Affairs
KATHRYN SCHULTZ
Director, Government Affairs
312-926-6961
MIKE WEAVER
Chairman, House of Delegates
815-599-6113
mweaver@fhn.org
ANA FERNANDEZ
Technician Representative
312-926-6980
DAVID TJHIO
Chairman, Committee on Technology
816-885-4649
david.tjhio@cerner.com
BRANDI STRADER
Chairman, New Practitioners Network
217-544-6464
JACOB GETTIG
Editor & Chairman, KeePosted Committee
630-515-7324 fax: 630-515-6958
jgetti@midwestern.edu
SCOTT MEYERS
Executive Vice President, ICHP Office
815-227-9292
scottm@ichpnet.org
Regional Directors
NOELLE CHAPMAN
Regional Director North
312-926-2547
nchapman@nmh.org
LYNN FROMM
Co-Regional Director South
618-391-5539
TARA VICKERY-GORDON
Co-Regional Director South
618-643-2361 x2330
JULIA SAPOZHNIKOV
Student Chapter Liaison
University of IL C.O.P.
sapozhn1@uic.edu
NEHA KAPUR
President, Rockford Student Chapter
University of IL C.O.P.
kapur4@uic.edu
CAROLYN TOY
President, Student ChapterMidwestern University C.O.P.
ctoy59@midwestern.edu
MARIA LAURA ITUAH
President, Student Chapter
Chicago State University C.O.P.
mituah@csu.edu
KIMBERLEE KABBES
President, Student Chapter
Southern Illinois University Edwardsville S.O.P
kikabbe@siue.edu
COURTNEY MAKOWSKI
President, Student Chapter
Roosevelt University C.O.P.
Welcome New Members!

| New Member |
Recruiter |
| Susan Laird |
|
| Jeremy Moretz |
Alicia Juska |
| Marie Tucker |
|
| Lawrence Sanchez |
|
| Jordan Faison |
Christine Lo |
| Brett Dunham |
Christine Lo |
| Patrick Prunty |
|
| Kathleen DeSmith |
Charles Pierce |
| April Switzer |
Charles Pierce |
| Adit Shah |
|
| Eva Pietraszek |
Jill Warszalek |
| Kristine Ficarella |
Chris Qullian |
| Florence Patino |
|
ICHP Pharmacy Action Fund (PAC) Contributors
Names below reflect donations between April 1, 2014 and April 1, 2015. Giving categories reflect each person's cumulative donations since inception.
ADVOCACY ALLIANCE - $2500-$10000
Kevin Colgan
Edward Donnelly
Dave Hicks
Frank Kokaisl
Michael Novario
LINCOLN LEAGUE - $1000-$2499
Scott Bergman
Andrew Donnelly
Ginger Ertel
Linda Fred
James Owen Consulting Inc.
Ann Jankiewicz
Jan Keresztes
Kathy Komperda
Despina Kotis
William McEvoy
Scott Meyers
Michael Rajski
Edward Rickert
Christina Rivers
Michael Short
Carrie Sincak
Miriam Mobley-Smith
Avery Spunt
Michael Weaver
Patricia Wegner
Thomas Westerkamp
CAPITOL CLUB - $500-$999 Sheila Allen
Margaret Allen
Rauf Dalal
Drury Lane Theater
Ann Jankiewicz
Leonard Kosiba
George MacKinnon
Janette Mark
Mary Lynn Moody
Jennifer Phillips
Edward Rainville
JoAnn Stubbings
UIC Student Chapter
Jill Warszalek
GENERAL ASSEMBLY GUILD - $250-$499 Tom Allen
Pete Antonopoulos
Peggy Bickham
Jaime Borkowski
Sandra Durley
Nancy Fjortoft
Michael Fotis
Travis Hunerdosse
Zahra Khudeira
Ann Kuchta
Mary Lee
Gloria Meredith
Justin Schneider
Kathryn Schultz
Kristi Stice
Heidi Sunday
Alan Weinstein
SPRINGFIELD SOCIETY - $100-$249
Jen Arnoldi
Jerry Bauman
Jill Borchert
Donna Clay
Mark Deaton
John Esterly
Gireesh Gupchup
Joann Haley
Joan Hardman
Glenna Hargreaves
Charlene Hope
Robert Hoy
Diana Isaacs
Kim Janicek
Stan Kent
Kati Kwasiborski
Kristopher Leja
George Lyons
Ronald Miller
New Practitioners Network
Karen Nordstrom
Peggy Reed
Katie Ronald
Brandi Strader
Jennifer Tryon
Tara Vickery-Gordon
Carrie Vogler
Marie Williams
Cindy Wuller
William Wuller
GRASSROOTS GANG - $50-$99
Brett Barker
Gunchoo Chadha
Jeanne Durley
Mary Eilers
Lara Ellinger
Clara Gary
Carol Heunisch
Brian Hoff
Mike Koronkowski
Kim Lim
Mark Luer
Bella Maningat
Milena McLaughlin
Megan Metzke
Katherine Miller
Julio Rebolledo
Mark Ruscin
Stacy Schmittling
Evanna Shopoff
Lucas Stoller
Dave Willman
Janeen Winneke
Amanda Wolff
CONTRIBUTOR - $1-$49
Renee Advincula
Yinka Alaka
Anchalee Ardharn
Lisa Ball
Roger Ball
Marci Batsakis
Greg Biedron
Amy Boblitt
Kathy Cimakasky
Mardhia Dayisi
Andreea Ducu
Veronica Flores
Deb Fox
Janice Frueh
Crystin Gloude
Linda Grider
Alisa Groesch
Rebekah Hanson
Margaret Heger
Ina Henderson
Julie Kasap
Dijana Keljalic
Nehrin Khamo
Josephine Kochou
Huda-Marie Kuttab
Irvin Laubscher
Chris Little
Kristopher Lozanovski
Laura Mazzone
Kit Moy
Syed Munawer
Whitney Palecek
Hina Patel
Abby Reeder
Cheryl Scantlen
Elba Sertuche
Hannah Sheley
Chris Shoemaker
Carrie Silverman
Theophilus Simon
Jennifer Splawski
Gloria Sporleder
David Tjhio
Zakarri Vinson
Michael Wilcox
Christina Yates
Thomas Yu
Upcoming Events

Thursday, April 2
LIVE Program! It Pains Me to Say It: The Role of IV Acetaminophen in Perioperative Pain Management
Pharmacist and Technician-specific WCSHP CPE Program
OSF Saint Francis Medical Center | Peoria, IL
Tuesday, April 14
LIVE Program! Edoxaban: The New Kid on the Block and Where it Fits with Existing Oral Anticoagulant Therapy
Pharmacist-specific CPE Sangamiss Program
PAO Bistro | Springfield, IL
Thursday, April 30
LIVE Program! Basal Insulin Therapy in the Treatment of Insulin Resistant Type 2 Diabetes: The Role of the Pharmacist in Ensuring the Safe and Effective Use in Patients
Pharmacist-specific CPE NISHP Program
Maggiano's | Oakbrook, IL
New Practitioners Network & Pharmacy Directors Network Night at the Ballpark
Chicago Cubs vs. Washington Nationals
Wrigley Field | Chicago, IL
Wednesday, July 1
Submission Deadline! 2015 Best Practice Award Entries
Thursday, July 16
SSHP Night at the Ballpark
Springfield Sliders vs. West Virginia Miners
Springfield Sliders Baseball Club | Springfield, IL
Thursday, September 10 - Saturday, September 12
ICHP 2015 Annual Meeting
Pharmacist & Technician-specific CPE programming
Drury Lane Conference Center | Oakbrook Terrace, IL

Print Entire Issue