Official Newsjournal of the Illinois Council of Health-System Pharmacists

November 2021
Volume 47 Issue 4

Features
2017 Best Practice Award Winner
Columns
College Connection
University of Illinois at Chicago (Rockford)
More
Officers and Board of Directors
ICHP Pharmacy Action Fund (PAC) Contributors
KeePosted Info

Loves Park, IL 61111-8653
Phone: (815) 227-9292
Fax: (815) 227-9294
ichpnet.org
Ad Submission Information and Deadlines (here): http://www.ichpnet.org/resources/keeposted_submission.php
KeePosted
Official Newsjournal of the Illinois Council of Health-System Pharmacists
EDITOR
Jennifer Phillips
ASSISTANT EDITOR
Milena McLaughlin
MANAGING EDITOR
Scott Meyers
ASSISTANT MANAGING EDITOR
Trish Wegner
DESIGN EDITOR
Leann Nelson
EXECUTIVE VICE PRESIDENT
Scott Meyers
VICE PRESIDENT - PROFESSIONAL SERVICES
Trish Wegner
DIRECTOR OF OPERATIONS
Maggie Allen
INFORMATION SPECIALIST
Heidi Sunday
CUSTOMER SERVICE AND
PHARMACY TECH TOPICS™ SPECIALIST
Jo Ann Haley
ACCOUNTANTS
Jan Mark
COMMUNICATIONS MANAGER
Leann Nelson
ICHP Mission Statement
Advancing Excellence in Pharmacy
ICHP Vision Statement
ICHP dedicates itself to achieving a vision of pharmacy practice where:
- Pharmacists are universally recognized as health care professionals and essential providers of health care services.
- Patients are aware of the training, skills, and abilities of a pharmacist and the fundamental role that pharmacists play in optimizing medication therapy.
- Formally educated, appropriately trained, and PTCB certified pharmacy technicians manage the medication distribution process with appropriate pharmacist oversight.
- Pharmacists improve patient care and medication safety through the development of effective public policies by interacting and collaborating with patients, other health care professionals and their respective professional societies, government agencies, employers and other concerned parties.
- Evidence-based practices are used to achieve safe and effective medication therapies.
- There are an adequate number of qualified pharmacy leaders within the pharmacy profession.
- Pharmacists take primary responsibility for educating pharmacy technicians, pharmacy students, pharmacist peers, other health professionals, and patients about appropriate medication use.
KeePosted Vision
As an integral publication of the Illinois Council of Health-System Pharmacists, the KeePosted newsjournal will reflect its mission and goals. In conjunction with those goals, KeePosted will provide timely information that meets the changing professional and personal needs of Illinois pharmacists and technicians, and maintain high publication standards.
KeePosted is an official publication of, and is copyrighted by, the Illinois Council of Health-System Pharmacists (ICHP). KeePosted is published 10 times a year. ICHP members received KeePosted as a member benefit. All articles published herein represent the opinions of the authors and do not reflect the policy of the ICHP or the authors’ institutions unless specified. Advertising inquiries can be directed to ICHP office at the address listed above. Image disclaimer: The image used in the Pharmacy Tech Topics™ advertisement is the property of © 2017 Thinkstock, a division of Getty Images.
Copyright © 2017, Illinois Council of Health-System Pharmacists. All rights reserved.
 Presidents Message
Presidents Message
President’s Year End Summary
by Charlene Hope, PharmD, MS, BCPS, ICHP President
In 1929 Frigyes Karinthy suggested that a chain of "a friend of a friend" statements could be made to connect any two people in a maximum of six steps. It is the basis of the theory of the “six degrees of separation,” which is the idea that all living things and everything else in the world are six or fewer steps away from each other. I often recall an interaction from many years ago, early in my career when I attended an ASHP Midyear Meeting in Atlanta, GA. I had run into my former Residency Director on my way to an educational session, and we started catching up on our lives over the last couple of years. He shared with information regarding a pharmacist in another state who he thought I might had known due to a mutual acquaintance that we both knew in Illinois. From what I remember, the information he shared with me about that pharmacist was not exactly positive. As we said our goodbyes, I reflected on the conversation and was fascinated by how connected we are in pharmacy through pharmacy school – our classmates, faculty and preceptors; and through residency training – our co-residents. residency preceptors, and other pharmacy staff members. Through the connections that we make as we navigate different careers or fields of pharmacy, we start developing connections that many of us may totally be unaware of. In pharmacy, and perhaps in part due to my active involvement in professional organizations, it has been long held belief of mine that within the pharmacy profession, it is more like “three degrees of separation” rather than six.
Seth Godin, a well-known marketer, entrepreneur and innovator coined the phrase “the connection economy.” The connection economy rewards value created by building relationships and fostering connections, rather than in an industrial economy where the value based on creating products or manufacturing things. This year, we embarked on a year of innovation, a year to focus on bringing new ideas that would increase the value of ICHP and moving those ideas forward to continue to foster the future success of ICHP.
One of those great ideas that came from the attendees of last year’s leadership retreat was finding ways to create and market the value of ICHP beyond continuing education (CE) offerings. During one of the brainstorming sessions, many of the attendees spoke to the face-face connections that kept them reminded as to why they became pharmacists and the importance of their ability to give back to profession. Throughout the year, there grew a need to create a space and foster new group formations within ICHP. The Division of Educational Affairs came together to incorporate new networking sessions into Annual Meeting agenda.
Attending the new networking session was one of the highlights for me of this year’s Annual Meeting. This session allowed interested attendees to meet and discuss topics important to them in a few key areas: Leadership, Ambulatory Care, Pharmacy Practice and Medication Safety. I joined the Medication Safety table, which consisted of a diverse group of both pharmacy technicians and pharmacists, senior level managers and newer practitioners/leaders entering this field as front-line pharmacists. It was wonderful to be able to share amongst the group not only challenges but strategies that have worked. Most importantly, I heard from several others after the session that it was good walking away with a feeling that we are not alone in the some of the struggles that we face in our organizations.
To me, the true value of ICHP membership goes beyond the high quality CE offerings. The value of ICHP resides in the abundant volunteer and professional development opportunities. It’s coming together to connect and share – the successes, the failures, the lessons learned – and at the end of the day knowing that we are not alone in our journey in providing the best care for our patients. It’s the people, the members, many of which, I feel I have “grown up” with professionally. The ones I know that I can call on for advice or direction when I need it. It’s about the great feeling you get after catching up with a former colleague who you see every year at the Annual Meeting but have known since the start of your career – and waving goodbye as you yell “See you next year!” across the parking lot.
It was truly an honor and a pleasure to serve as ICHP President over this past year. Thanks to all of you for your support, encouragement, hard work and dedication.
“Never doubt that a small group of thoughtful, committed citizens can change the world; indeed, it's the only thing that ever has.”
- Margaret Mead
 Directly Speaking
Directly Speaking
Pharmacy Month is a Great Time to Reach Out to Your Legislators!
by Scott A. Meyers, Executive Vice President; Kathryn Schultz, ICHP Treasurer and Christopher Crank, ICHP Government Affairs Director
October is National Pharmacy Month. October 15-21, 2017 is National Hospital and Health-System Pharmacy Week and Tuesday, October 17th is National Pharmacy Technician Day! It’s a great time to celebrate!
Governor Rauner just signed HB3462, the two-year extension of the Pharmacy Practice Act which creates a new Collaborative Pharmaceutical Task Force that will shape the Practice Act for the future! So why not use Pharmacy Month and all of its festivities to show your legislators just what a hospital or health-system pharmacist does? It’s important to get to know them now before you really need to ask them for a favor. So it’s easy to reach out to them but just in case you think you can’t do it, we’re going to show you how you can! And after we do, we’re going to tell you why every one of you needs to make this effort this year and this month!
To find your legislators and set up a visit:
[Note: If you are reading this article online, skip directly to clicking on the hyperlink in step 3. If you are reading a hardcopy of KeePosted, start with step 1.]
- Go to the ICHP website: http://www.ichpnet.org and place your cursor over the Pharmacy Practice Tab.
- Click on the Advocacy button.
- Click on the link titled Advocacy Center just below the picture on that page.
- Locate the Find Officials box on the right hand side and type in your zip code. You will then need to type in your street address as many zip codes are split by district boundaries.
- The results will contain a list of both your Federal and State elected officials.
- Click on your State Senator or State Representative, and you will find a comprehensive bio that includes contact information. Most of the bios provide an email address but a few may not.
- For those entries that do not provide an email address, you may try to find them on the Illinois General Assembly website at www.ilga.gov
- There click on “Members” under Senators or under Representatives to look up any incomplete information about your legislator. You may still not find an email address, so written communication or a phone call will have to do.
- From either source, find your legislators “District” office, not the Springfield office.
- However, if the legislator provides an email address, then that is their preferred means of contact. If they don’t provide one, then old school is the ticket with a phone call or better yet a written (on your computer so they can read it) letter.
- To visit them in their office, call and set up an appointment in advance. Dropping in on them in the district is strongly discouraged plus they are very seldom there anyway.
- When meeting your legislator:
- Dress professionally!
- Introduce yourself and provide your address. This lets them know you’re a constituent without having to say it. In addition, they may know one or more of your neighbors which is a great conversation starter.
- Be polite. Always!
- Be concise and speak in layman’s terms. They most likely do not have a health care background.
- Offer to help them with any health care related bill information (especially pharmacy, of course).
- Join their email group if they have one and/or follow them on Facebook.
- Get permission from your hospital community relations department and invite them to come visit your pharmacy during Pharmacy Month to see what a hospital/health-system pharmacist does!
- Follow up with their assistant to set up the visit details. Perhaps even make it into a group visit and have multiple legislators visit together.
- Follow up with your legislator after their visit and ask if they have any questions about the visit or if there is something you can help them with regarding any healthcare legislation.
- Post your story and/or pictures on the ICHP Facebook page (offer to send them to your legislator too as many of them love the PR!).
- Consider contributing to your legislator’s campaign fund or political action committee. This shows your sincere support for them.
Hopefully, that doesn’t sound too hard. So now, here’s why we need your help. The Collaborative Pharmaceutical Task Force will be appointed by the following legislative leaders and made up of representatives from the following organizations:
The Speaker of the House, Michael Madigan shall appoint:
The Illinois Retail Merchants Association Representative
The Chairman of the Task Force
The President of the Senate, John Cullerton shall appoint:
The Illinois Pharmacists Association Representative
A representative of a statewide organization representing unionized pharmacy employees
The Minority Leader of the House, Jim Durkin shall appoint:
The Illinois State Medical Society Representative
The Illinois Council of Health-System Pharmacists Representative
The Minority Leader of the Senate, Bill Brady shall appoint:
The Illinois Hospital Association Representative
A representative of a statewide association representing long-term care pharmacists.
In addition, the Secretary of the Department of Financial and Professional Regulation, Bryan Schneider shall appoint the following non-voting members of the Task Force:
A representative of the University of Illinois at Chicago, College of Pharmacy
A clinical pharmacist with extensive study in pharmacy e-prescribing
A representative of the Department
You can see that the Task Force has a wide-ranging membership, and a broad scope of interests are represented. This means that health-system pharmacy will need to be heard not only at the Task Force table but with all of Illinois’ legislators as soon as deliberations begin. We encourage all of our members to take a look at Public Act 100-0497 and especially Section 85/4.5 The Collaborative Pharmaceutical Task Force, to see what is in store. But that section only describes what is statutorily mandated to be discussed by the Task Force. The entire Act will be open for discussion, and ICHP’s Government Affairs Division has been reviewing it in its entirety and have put together a variety of changes that would bring the Act up to today’s highest practice standards.
So our request to you each of you is to “Reach Out” to your State Senator and State Representative and show them what hospital and health-system pharmacists do every day. Show them where the Act limits your ability to practice at the top of your clinical ability. Show them that you want to help them make Illinois a healthier and safer State for all of its citizens and your patients! Pharmacy Month is a great time to reach out to your legislators!
Features
2017 Best Practice Award Winner
Implementation of Integrated Telepharmacy Services Achieve a Health-System Standard of Pharmacy Care
Feature Article
by Sandra M. Salverson , PharmD, BCPS and Jerry Storm, RPh

WINNER

The 2017 Best Practice Award Winner, Implementation of Integrated Telepharmacy Services Achieve a Health-System Standard of Pharmacy Care, is available as a home-study for CPE credit. To earn your CPE credit, you must read the manuscript below in the September/October 2017 issue of KeePosted and then go toCEsally.com to answer the self-assessment questions and complete your credit. Once you have logged in to your CEsally.com account, search on Implementation of Integrated Telepharmacy, add to your To Do List, be sure and save CE, and then go to your To Do List to complete the process. If you have questions on how to set up your CEsally account, please call the ICHP office at 815-227-9292.
Peoria, IL
OSF Healthcare System
Target Audience
- Identify three functions ePharmacists can perform within a telepharmacy model.
- Recognize one clinical outcome and one dispensing outcome from integrating telepharmacy services into a health-system model of pharmacy care.
- Identify the role of the pharmacy technician in a pharmacy model with integrated telepharmacy services.
- Recognize the impact 24/7 pharmacist prospective review of medication orders has on dispensing doses from night-rooms.
 This program is provided by the Illinois Council of Health-System Pharmacists. The Illinois Council of Health-System Pharmacists is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education. This program is equivalent to 0.5 contact hour (0.05 CEU) of pharmacy continuing education.
This program is provided by the Illinois Council of Health-System Pharmacists. The Illinois Council of Health-System Pharmacists is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education. This program is equivalent to 0.5 contact hour (0.05 CEU) of pharmacy continuing education.
Introduction
Many health-systems participate in quality care and/or value-based reimbursement programs. The commitment to sharing risk within payment models means if quality care is provided, health-systems will receive reimbursement for those achievements. If quality care is not provided, payment received will continue to decline the more the target is missed. This change in the reimbursement model has healthcare-systems searching for ways to achieve significant financial efficiencies and improve quality. Mergers and acquisitions continue to occur in response to the need for economies of scale. As a result, many health-systems now contain a blend of hospital sizes.
The costs of both appropriate medication use and suboptimal medication use comprises approximately 10% of the total dollars spent in the United States.1 Optimizing medication use within a health-system is collaborative and requires partnerships across disciplines and geographies of the health-system.2 In 2013, a survey of pharmacy services in small and rural hospitals in Illinois demonstrated approximately 23.5% - 31% use a drug-distribution model of care and approximately 50% deliver patient-specific clinical services the majority of time.3 Another study4 reported rural facilities, defined as an average daily census of 49 or fewer inpatients, were less likely than larger hospitals to demonstrate safe medication practices and were less likely to support a full-time pharmacist due to limited patient volume and/or lack of financial resources. The pharmacy enterprise needs to advocate for and optimize the value of drug therapy and medication use safety. The challenge within the large health-system models is to implement these solutions consistently across an entire enterprise that contains tertiary-referral medical centers, rural community hospitals, and critical access hospitals.
Purpose/Goal
The aim of the health-system is to provide consistent quality care for people in the communities they live. In 2012, the health-system opted to pursue an operating organizational structure to manage care for patient populations, enhance decision making, increase agility, increase service consistency, improve clinical care, and improve cost management. In 2014, health-system administration asked pharmacy services to functionally transform. In lieu of operating independent pharmacy departments within each respective hospital, the objective was to form one operational department for the entire health-system and to optimize service delivery. Using the existing human resources, administration requested pharmacy services design a model of care that ensured all patients have access to the same level of pharmaceutical care, improved patient outcomes, and improved medication outcomes associated with the medication use process.
Description of the Program
The health-system includes eleven hospitals in urban and rural settings: one tertiary referral medical center with a children’s hospital, six community hospitals, and four critical access hospitals. The health-system shares the same electronic medical record with computerized provider order entry and bar-code medication administration. Two-thirds of the hospitals used automated dispensing cabinets as the core medication distribution system.
Senior pharmacy leadership conducted interviews with administrators, pharmacy leaders, nursing leaders, medical staff involved in pharmacy and therapeutics work, and pharmacists across the health-system to determine 1) what medication use and pharmacy practices are evidence-based and effective and 2) the top concerns/gaps in care. Table 1 reports the results of the gap analysis and top priorities identified. The redesigned pharmacy practice model recommended all hospitals include: around-the-clock order verification, around-the-clock emergency department order verification, patient education, discharge medication reconciliation review, antimicrobial stewardship, and focused pharmacy dosing services.
Table 1. Pharmacy Services Gap Analysis and Care Model Priorities Pre and Post-Functional Transformation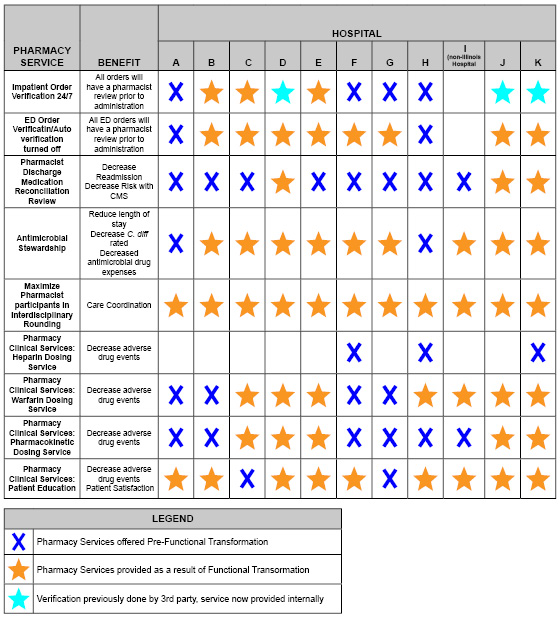
The new model of pharmacy care implemented centralized patient care services through ePharmacy, a virtual telemedicine service. ePharmacists prospectively verify orders around-the-clock for every single hospitalized patient within the health-system. ePharmacists review discharge medication reconciliation and identify potential errors in both the visit summary and discharge scripts to prevent adverse events and readmissions prior to every patient’s discharge. ePharmacists also manage first-dose consults for antibiotics and warfarin (under the auspices of collaborative drug therapy management (CDTM) agreements with each hospital’s independent medical staff). Pediatric ePharmacy, supported by the health-system’s children’s hospital, manages the health-system’s pediatric orders, consults, and discharge medication reconciliation review. Pharmacists and technicians on-site at the hospitals are responsible for medication distribution and medication compounding. Pharmacists at the hospital sites educate patients receiving any oral anticoagulants, participate in interdisciplinary rounds, practice antimicrobial stewardship services, and perform the daily consult dosing services for antibiotics, warfarin, and heparin (under the auspices of CDTM agreements). Pharmacists functioning located at the critical access hospitals function in a hybrid model. The provide telepharmacy services for the entire health-system and the services expected for site pharmacists. Figure 1 below exhibits the model implemented.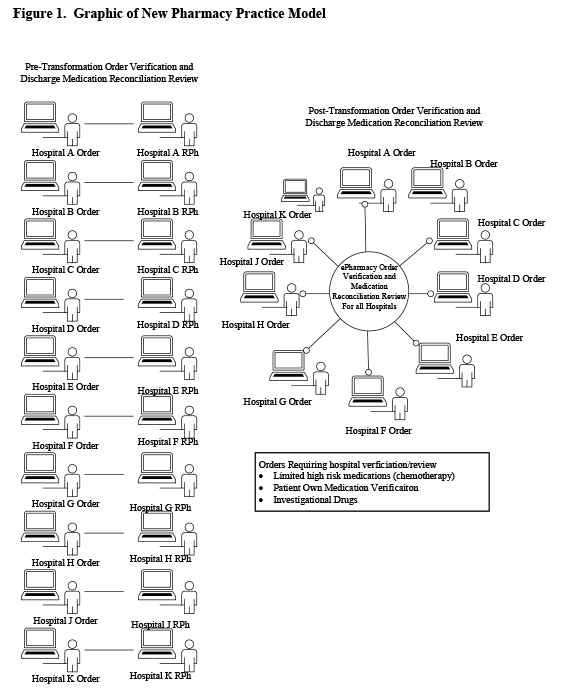
Execution of pharmacist prospective order review around-the-clock throughout the health-system allowed the development and implementation of a standard process for after-hours dispensing when a pharmacist is not physically present at a hospital. The objective was to minimize nurses’ need to use the after-hours night room/cabinet and almost completely eliminate the need for nurses to compound IV infusions when the pharmacist is not on-site. Medication distribution systems were aligned and implemented to maximize automated dispensing cabinet use. Automated dispensing cabinets are all profiled, with the exception of procedure areas. Override medication lists permitting bypass of prospective pharmacist review were redesigned and limited to medications for patient emergencies.
Implementation of around-the-clock pharmacy services throughout the health-system granted full coverage of pharmacist managed dosing services offered. CDTM agreements were aligned and implemented for warfarin, heparin, vancomycin, and aminoglycosides.
Experience with and Outcomes of the Program
Order Verification and After-hours Dispensing Practices
Prior to the practice model change, average turn-around times for medication review and nursing access to medications in automated dispensing cabinets averaged 140 – 180 minutes for high priority orders, and 180 minutes for routine orders. Implementation of ePharmacy services yielded high priority order review with medications accessible in 15 minutes or less; routine orders review and medication access occurs in 60 minutes or less, consistently. Prospective pharmacist review of orders around-the-clock and re-design of the medication distribution system in hospitals without an around-the-clock pharmacist physically present resulted in a 95% absolute reduction in the number of non-automated dispensing cabinet dispenses during pharmacy closed hours. Nurse compounding of sterile preparations decreased by 87%. Table 2 summarizes the changes in doses dispensed by nurses after-hours. It eliminated the need for nurses to enter the pharmacy after-hours.
Table 2. Changes in Doses Prepared and Dispensed by Nurses After-Hours
| Mean Number of Non-Automated Dispensing Cabinet Doses Dispensed | Mean Number of Nurse Compounded Sterile Preparations | |
| Pre-Pharmacy Practice Model Change (Oct 15 - Mar 15) | 500 | 33 |
| Post-Pharmacy Practice Model Change (Oct 16 - Mar 17) | 25 | 4 |
Pharmacist Discharge Medication Reconciliation Review
Discharge medication reconciliation review was a standard of care within the health-system prior to the model changes. Pre-transformation, pharmacists reviewed 65% of patients discharged. Post-transformation, ePharmacists review 97% of patients discharged. ePharmacists identify at least one drug related problem (drug-drug interaction, drug duplication, inappropriate dose, inappropriate duration, or undertreated condition) and correct the problem(s) for twenty percent of patients immediately prior to discharge. Examples of problems identified and resolved include: omission of anti-hypertensives for a patient admitted for hypertensive crisis, omission of anti-platelet agent for post-myocardial infarction, duplicate prescriptions for rivaroxaban with two unique set of instructions to start on same day, and unnecessary continuation of antibiotics when the course of therapy was documented as complete.
Anticoagulation Management
Prior to aligning into one operational department, 50% the hospitals offered pharmacist managed warfarin services. After the operational alignment, all hospitals offer anticoagulation management. The service manages 80% of the warfarin patients within the health-system. Toxicity, as defined by an INR greater than 4.5, began at 0.7% and averages 2.0% post model and patient load increase. Toxicity for patients not managed by pharmacy began at 4.3% and now averages 2.9% for the entire health-system. Overall the health-system maintains a toxicity rate of 2.2% (Figure 2).
Figure 2. Critical INRs for the Health-System

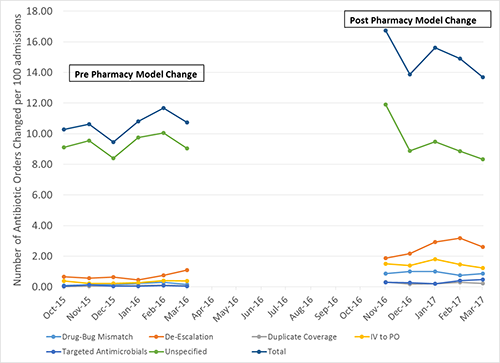
Antimicrobial Stewardship
During the time of the model change, a system-wide antimicrobial stewardship program was implemented. Two infectious disease pharmacotherapists mentor and guide pharmacists at each hospital to perform targeted interventions: drug-bug mismatch, de-escalation, duplicate coverage, and intravenous to oral conversions. Figure 3 summarizes the number of documented changes to antimicrobial orders pre- and post-model change. Overall antibiotic use decreased 0.9% across the health-system.
Figure 3. Accepted Antimicrobial Stewardship Pharmacist Recommendations
Patient Education
Patient education was not a priority for pharmacists within the health-system. Centralized order verification allows more pharmacists to leave the pharmacy and interact with patients. A goal was set to educate patients receiving any oral anticoagulants (warfarin or a direct thrombin inhibitor) prior to discharge. Pharmacists now educate 75-85% (410 – 450 patients/month) of patients receiving an oral anticoagulant. This meets both the Joint Commission National Patient Safety Goal expectations and targets one of the health-system’s high risk populations for readmissions.
Clinical Outcomes
Pharmacist documentation of drug-related problems and resolution was an expectation throughout the health-system. Pharmacist document recommendations using the taxonomy described by Hoth et al.5 Figure 4 summarizes the difference in drug problems identified and resolved pre and post model change. The identification and prevention of adverse drug related events (allergy, management of actual adverse drug event, drug-drug interaction, drug-disease interaction, contraindication, therapeutic monitoring for toxicity, or lack of standard preventive care) did not change substantially. Optimization of medication therapies (no indication, untreated condition, undertreated condition, alternative therapy, minimal/no therapeutic effectiveness, dose adjustments for organ dysfunction, duplicate therapy or inappropriate schedule), excluding medications associated with a CDTM agreement, increased by 167%.
Figure 4. Resolution of Drug Related Problems Associated with the New Pharmacy Practice Model

Discussion of Innovative Aspects of the Program and Achievement of Goals
There are very few descriptions of how the integration of a comprehensive around-the-clock telepharmacy service impacts an entire health-system’s ability to meet the critical requirements for health-system pharmacy practice6-10, as outlined in the ASHP Pharmacy Practice Model Summit.11 Remote review of medication orders by pharmacists when the hospital pharmacy is closed has demonstrated a decrease in the number of potential adverse events reported within critical access hospitals.7-9 A pharmacist-managed reconciliation service using telepharmacy demonstrated improved discharge medication lists and documentation received by patients.10 The experiences published thus far report benefit to the critical access hospitals and do not describe an integrated health-system approach. The ASHP statement published in May 2017 calls for further research to be conducted to establish best practices.12
The integration of a centralized telepharmacy service into the health-system practice model allowed for expanded pharmacy services for a broad range of hospital sizes and types without the addition of additional resources. The integrated model achieved patient centered outcomes and correction of prescribing errors and drug related problems, similar to Sankaranarayanan et al.8 The model demonstrated outcomes at all hospitals and was not limited to the critical access hospitals alone. The model allows the provision of specialized services (pediatrics, antimicrobial stewardship) and expertise that typically would not be robustly implemented within the critical access and small rural hospital setting.3-4 All hospitals now have the ability to provide recommended pharmaceutical care for all patients: medication reconciliation, review of orders before administration of the first dose, individualized treatment and monitoring plans, provision of patient education, daily drug monitoring, and participation in patient care rounds. The health-system also delivers consistent services for high-risk patients as well: anticoagulation management, antimicrobial stewardship, streamlined medication orders, pharmacokinetic evaluation, monitoring, and dosing, and renal dose adjustments.
Conclusion
Integrated telepharmacy services with the redistribution of pharmacist resources increased patient access to pharmacists. The new model yields consistent pharmacy services throughout one health-system, identifies and resolves more drug-related problems than the previous federated model.
References
- National Center for Health statistics, Center for Disease Control and Prevention. Health expenditures (2014 data). https://www.cdc.gov/nchs/fastats/health-expenditures.htm (accessed 2017 Jun 17).
- Knoerr, S. Stewardship of the pharmacy enterprise. Am J Health-Syst Pharm 2014; 71:1204-9.
- Crawford SY, Schumock GT, Ursan JD, et al. Comparison of pharmacy services at critical access hospitals and other rural and small hospitals in Illinois. Am J Health-Syst Pharm 2013;70:1313-21.
- Cochran G, Jones K, Xu L, et al. Prevalence of evidence-based safe medication practices in small rural hospitals. RUPRI Center for Rural Health Policy Analysis. Rural Issue Brief. Brief No 2008-1. https://cph.uiowa.edu/rupri/publications/issuebriefs/IssueBrief2008-1.pdf (accessed 2017 Jun 17).
- Hoth AB, Carter BL, Ness J, et al. Clinical Pharmacist Recommendation Taxonomy Pharmacotherapy 2007;27(5):639-646.
- Garrelts JC, Gagnon M, Eisenberg C, et al. Impact of a telepharmacy in a multi-hospital health-system. Am J Health-Syst Pharm 2010;67:1456-62.
- Wakefield DS, Ward MM, Loes JL, et al. Implementation of a telepharmacy service to provide round-the-clock medication order review by pharmacists. Am J Health-Syst Pharm 2010;67:2052-7.
- Sankaranarayanan J, Murante LJ, Moffett LM. A retrospective evaluation of remote pharmacist interventions in a telepharmacy service model using a conceptual framework. Telemedicine and e-Health. 2014; 10(20): 893-901.
- Peterson CD, Rathke A, Skwiera J, et al. Hospital telepharmacy network: delivering pharmacy services to rural hospitals. J Pharm Technol 2007; 23:158-65.
- Keeys C, Kalejayie B, Skinner M, et al. Pharmacist managed inpatient discharge medication reconciliation: a combined onsite and telepharmacy model. Am J Health-Syst Pharm 2014; 71:2159-66. Shane R. Critical requirements for health-system pharmacy practice models that achieve optimal use of medicines. Am J Health-Syst Pharm 2011; 68:1101-11.
- Alexander E, Butler CD, Darr A, et al. ASHP Statement on telepharmacy. Am J Health-Syst Pharm 2017; 74:e236-41.
2017 ICHP Annual Meeting
Award Winners and Photos!
Feature Article
Congratulations to all of the 2017 Award Winners! Thank you to all who attended and all who spoke. (view the award banquet photos)
2017 Shining Stars:
Julie Downen
Don Ferrill
Brian Cryder
Heather Harper
Hailey Soni
Ehsan Tavassoli
Tamkeen Abreu
Bernice Man
Kathryn Schultz
David Martin

Outstanding Volunteer of the Year Award:
Abir (Abby) Kahaleh
New Practitioner Leadership Award:
Lara Ellinger
Mary W. Lee
Pharmacist of the Year Award:
Despina Kotis
Student Chapter Award:
University of Illinois at Chicago College of Pharmacy
Technician of the Year:
Clara Gary
President’s Award:
Carrie Vogler
Immediate Past President Award:
Charlene A. Hope
For more information about each award, go to the awards page on the ICHP website at http://www.ichpnet.org/members/award_winners/
Columns
Board of Pharmacy Update
Highlights of the September Meeting
by Scott A. Meyers, Executive Vice President
The September 12th Board of Pharmacy Meeting was held at the James R. Thompson Center at Randolph Street and LaSalle Street in downtown Chicago. These are the highlights of that meeting.
Department Update – Katy Straub, Board of Pharmacy’s general counsel provided news from the Department of Financial and Professional Affairs. The Department is now collecting all licensee email addresses as this will be the preferred method of communication in the future.
Patient Counseling Rules went into effect on August 18th with enforcement going into effect on September 1st. Pharmacists or student pharmacists must provide counseling to patients whenever a new patient present a prescription, an existing patient presents a new prescription, or an existing patient presents a change in dose, frequency or route of an existing prescription. Pharmacy Technicians may no longer provide an offer for counseling. A sign must be clearly posted near the cash register or patient waiting area describing the patient’s right to counseling. The sign may be downloaded from the Department’s website. If counseling is not practicable as in cases of mail order, home prescription delivery or in the professional judgement of the pharmacist, a copy of the sign must be placed in the bag or envelope containing the filled prescription. If a pharmacist is on a lunch break and unavailable to counsel, no medications may leave the pharmacy.
Licensing of all new pharmacy technicians must be done online now with no mailed paper applications accepted by the Department. All communications regarding the licensing process will be done online also. This will eliminate the deficiency letter process and will provide the applicant with immediate feedback when an application is deficient.
The 2017 NABP District IV Meeting – will take place in Toledo, Ohio in early November. The meeting is jointly sponsored by the Ohio Board of Pharmacy and the University of Toledo College of Pharmacy. Illinois will be represented by several Board members and a variety of faculty from Illinois’ six colleges of pharmacy.
Legislative Update – was provided by IPhA Executive Director, Garth Reynolds. The bills described are also highlighted in this issues Government Affairs Report. The November update will be provided by ICHP’s Executive Vice President.
Audience Comments – At the conclusion of the open portion of the Board meeting, members of the audience are allowed to ask questions and provide comments to the Board members. During this portion, there were several questions clarifying the counseling rules requirements. For example, what to do if the patient sends a neighbor or family member to pick up their prescriptions and the pharmacist believes this may create a HIPAA violation. The pharmacist always has the ability to use his/her professional judgement and determine that counseling is not practicable in a specific case. The sign is then required to be included in the bag, and it was suggested that the pharmacist should reach out to the patient proactively to make sure he/she understands the important aspects of their medication therapy.
The Department staff was asked when the draft compounding rules would be published, and it was reported that it would be soon. We’re not sure how “soon” is defined but sometime this fall.
Next Board of Pharmacy Meeting – The next meeting of the Illinois Board of Pharmacy will be held at 10:30 AM on Tuesday, November 14th at the James R. Thompson Center in downtown Chicago. Announcements and agendas are posted at least 14 days in advance on the IDFPR pharmacy website. The profession is welcome to attend the open portion of this meeting.
Educational Affairs
Call for Posters - Deadline January 10, 2018
Are you working on a project that others could learn from? Please consider sharing the outcomes with your colleagues at the poster session during the ICHP Spring Meeting April 13-14, 2018 in East Peoria, IL! This is a great opportunity to share innovative ideas with others and learn about trends in Illinois health-system pharmacies. All ICHP members are eligible to submit abstracts to be considered for presentation at the Spring Meeting.
Click here for all the details.
Categories for submission:
Original Research: To be considered for acceptance, papers must describe original research in pharmacotherapeutics, clinical pharmacokinetics, pharmacodynamics, practice innovations in organized health-care settings, administrative practice or cost analysis of pharmaceutical services. Papers must not have been published in abstract or complete form or have been presented elsewhere prior to presentation at the ICHP Spring Meeting.
Research in progress: To be considered for acceptance, papers must describe original research in progress in pharmacotherapeutics, clinical pharmacokinetics or pharmacodynamics or practice innovations in organized health-care settings, administrative practice or cost analysis of pharmaceutical services. Papers must neither have been published in abstract or complete form nor have been presented elsewhere prior to presentation at the ICHP Spring Meeting. Those abstracts submitted as research in progress are expected to have results and conclusions available for poster presentation at the Spring Meeting. Those with no results and conclusions by the time of the meeting are disqualified.
Encore: Research may have been presented elsewhere or published in abstract or complete form only prior to presentation at the ICHP Spring Meeting. To be considered for acceptance, papers must describe research in pharmacotherapeutics, clinical pharmacokinetics, pharmacodynamics, practice innovations in organized health-care settings, administrative practice or cost analysis of pharmaceutical services. Posters or papers presented before January 1 of the previous year are not eligible. For example, posters or papers presented before January 1, 2017 are not eligible for 2018 submissions. Full results and conclusions must have been presented/published previously to qualify as an encore presentation. Those projects previously presented/published without results and conclusions should be submitted as an original poster.
Student: Only original material will be considered. Any material that has already been presented should be entered as an encore presentation. The person primarily responsible for the work must be a current student enrolled in an Illinois School of Pharmacy and must present the poster at the meeting.
Original research may be submitted as research in progress. Those abstracts submitted as research in progress are expected to have results and conclusions available for poster presentation at the Spring Meeting. Those with no results and conclusions by the time of the meeting are disqualified.
**Case reports and literature reviews are not eligible for poster submission. These types of research may be eligible for submission to ICHP's Newsjournal, KeePosted.
Platform Presentations
Abstracts submitted in the Original Research
category will be eligible for a platform presentation, as decided by the ICHP
Educational Affairs Division Poster Review Committee. The two abstracts
with the highest scores, submitted in the original research category with
results and conclusions at the time for abstract submission, will be invited to
participate in the platform presentation session at the Spring Meeting.
Each presentation will be 15 minutes in length.
Eligibility Criteria:
All Illinois health-system pharmacy practitioners, including pharmacists, pharmacy residents, pharmacy technicians, and pharmacy students are invited to submit projects for consideration. The submitting author must be a current ICHP member. If a student is listed as the submitting author for an original presentation, the poster will be eligible for the student award.
The submitting author should present the poster; however, if legitimate circumstances do not permit attendance at the meeting; another pharmacy professional author for that poster may present at the poster during the poster exhibit session at the Spring Meeting. All poster presenters must be registered for the Spring Meeting and complete ACPE required documents as requested, if the posters are accredited for continuing pharmacy education.
Submission:
Members wishing to submit a poster should use the online submission form. Be sure to click "Submit" after completing your form. The deadline for submissions is January 10, 2018. Please direct any questions to Trish Wegner at TrishW@ichpnet.org.
Deadlines:
Submission deadline is January 10, 2018. Authors will be notified of acceptance of their poster via email in February, 2018.
Government Affairs Report
The Governor’s Pen Has Been Busy
by Jim Owen and Scott Meyers
Late August and early September saw a plethora of bill signings by Governor Rauner. Here’s a summary of the few bills that were pharmacy related:
HB3462 – Now Public Act 100-0497 This is the big one, the revision/extension of the Pharmacy Practice Act. In addition to making many technical changes to bring the practice act in line with current practice, the bill creates the Collaborative Pharmaceutical Task Force, which will work on revising and updating the practice act over the next 12-18 months. The Task Force will consider workload issues along with e-prescribing as two important areas but will review the entire act to enhance its effectiveness. Effective Immediately.
HB313 – Now Public Act 100-0513 is a renewal of the Nurse Practice Act. The critical piece in this newly revised act is that after 4000 hours of clinical practice under a collaborative agreement with a physician, an Advanced Practice Nurse (APN) can apply to become an independent practitioner, no longer needing a collaborative agreement. This could create some interesting scenarios on the community pharmacy side. Effective January 1, 2018.
HB2531 – Now Public Act 100-0065 removes the requirement of generic pharmaceutical manufacturers to provide equivalency data to the Illinois Department of Public Health for the drug formulary. The drug formulary has not existed for several years as Illinois now defers to the FDA Orange Book. Effective Immediately.
HB2957 – Now Public Act 100-0138 This bill allows for synchronization of prescription refills and requires insurance providers to pay for the partial filling. It creates a pro-rated copay for the patient and requires the insurance provider to pay a full dispensing fee to the pharmacy. Effective Immediately.
SB1790 – Now Public Act 100-0237 allows pharmacies to provide a 30-day supply of an expired prescription (not including controlled substances) if the prescribing physician has abruptly retired or died. This gives the patient a chance to line up a new physician and not interrupt medication therapy. Effective Immediately.
SB1944 – Now Public Act 100-0326 revises the Hypodermic Syringes and Needles Act to now allows pharmacies to sell up to 100 needles and syringes without a prescription rather than the previous 20. This will provide patients with more options when insurance doesn’t cover the purchase of needles and syringes. Effective January 1, 2018.
These were the big bills this past legislative session. While there is no evidence that any significant pharmacy-related legislation will be introduced or acted upon during the fall veto session, we will be monitoring it closely. More importantly, we will continue to update you on the progress and discussions of the Collaborative Pharmaceutical Task Force and the potential revisions to the practice act as they occur.
Take the time this fall to visit with your local legislators and let them know that you’re available to assist them on any health care related issue they may have. Most importantly, get to know them before you have to ask them for a favor in the future!
ICHPeople

ICHP Members Represented ICHP at the Chicago AHA Heartwalk on September 23, 2017 (http://facebook.com/ichpnet)
Leadership Profile
Meet Milena McLaughlin, PharmD, MSc, BCPS-AQ ID, AAHIVP

What is your current leadership position in ICHP?
Ø I am the Secretary of NISHP and the Assistant Editor of KeePosted™.
What benefits do you see in being active in a professional association such as ICHP?
Ø I am sure that most people answer this with the importance of giving back to the profession. One of the other important benefits is self-development. By being engaged in ICHP, I am able to call upon my strengths to lead others and seek mentorship from others when I identify an area for improvement that is creating a barrier for me. I am then able to identify other members to provide opportunities and become a mentor. This cycle of mentor/mentee becomes a way of giving back to the profession.
What initially motivated you to get involved in ICHP?
Ø During my training at MWU/NMH, I was encouraged to become engaged in pharmacy service. I was previously very involved in pharmacy organizations in both Pennsylvania and New York. ICHP seemed to be a natural extension of these organizations. The existence of the New Practitioner’s Network and the “openness” with which ICHP mentors welcome new members and encourage leadership opportunities provided a large amount of intrinsic motivation.
Where did you go to pharmacy school?
Ø University of the Sciences in Philadelphia
Where have you trained or worked?
Ø I completed my PGY-1 Pharmacy Residency in New York City and my ID Fellowship at Northwestern Memorial Hospital through Midwestern University. I have been on faculty at MWU with my clinical practice site at the Northwestern ID Center since 2013.
What special accomplishments have you achieved?
Ø When other kids wanted to be ballerinas and astronauts, I wanted to be a math teacher. But then I could not decide between math and science. The pharmacy profession is wonderful because it marries math and science. I am a pharmacist; however, I am technically also a math teacher since I teach pharmacokinetics. I think that is pretty special.
Describe your current area of practice and practice setting:
Ø I am an outpatient HIV/ID clinical pharmacist at a multidisciplinary hospital-based clinic. Pharmacists are very well integrated into the patient care model and we have a collaborative practice agreement as well as our own patient message line. We have multiple students that greatly extend our reach to see patients prior to their appointments and identify medication related issues.
What advice would you give to student pharmacists?
Ø It’s not what you know, it’s knowing what you don’t know and knowing where to look to find information about what you don’t know. It’s also who you know and cultivating those relationships.
Do you have any special interests or hobbies outside of work?
Ø I love to bake and craft, anything creative after being “science-y” all day! I was recently asked to make a birthday cake out of soda cans.
Do you have a favorite restaurant or food?
Ø Sushi!
What is your favorite place to vacation?
Ø This is a very hard question! I have been trying to get to all 50 states and I have about 7 left.
What is the most interesting/unique fact about yourself that few people know?
Ø I know how to fly a plane.
What 3 adjectives would people use to best describe you?
Ø Rare, tenacious, droll
New Practitioners Network
Another Trip around the Sun - NPN Year in Review
by Colleen Bohnenkamp, PharmD, BCPS, BCOP
It’s hard to believe it’s been nearly a year since I was inducted as the New Practitioner Network Chair at the 2016 Annual Meeting. While it’s bittersweet to pass the torch to our new leader, Bernice Man, I am feeling nostalgic in recapping the events and initiatives the NPN has participated in this past year.
We kicked off the year with our 3rd Annual participation in the Juvenile Diabetes One Walk in October along the Chicago Lakefront Trail. As Ron Santo was a huge supporter of the Juvenile Diabetes Research Fund (JDRF), there was such an electricity in the air as the Cubs were approaching their World Series Championship. As a team, we raised over $500 for the JDRF.
Fast forward to Spring, where the NPN participated in our 4th Annual Ronald McDonald House (RMH) Event, where we prepared and served brunch to the families staying at the RMH. This was the first year that we volunteered at the location in Hines, IL. It was an excellent turnout with a lot of student support. Additionally, we hosted our inaugural networking and educational dinner sponsored by Sanofi. We learned about the new PCSK9 inhibitor alirocumab over a delicious dinner at Sullivan’s Steakhouse in downtown Chicago. This event was very well attended by New Practitioners and we hope to continue this networking event in the future.
We welcomed many new residents and students to our committee this summer and hosted the 2nd Annual Residency Social. Over 25 Chicagoland residents met at Millennium Park to socialize, relax, and enjoy the Movie, La La Land.
Many new members have joined our E-board over the past year, and there has been renewed student involvement in our monthly conference calls. Our members have authored articles ranging from working in Thailand to lecturing at their alma mater.
I am truly honored to have had the opportunity to lead such dedicated and talented individuals and to collaborate with the entire ICHP Staff. Involvement in the NPN has fostered my leadership and organizational skills, kept me in touch with what’s happening within ICHP on an organizational level, reconnected me to the University level, and introduced me to organizational leadership.
If you are interested in becoming more involved with ICHP and are within 10 years of graduation, I invite you to join us at some of our upcoming events:
- Ronald McDonald House Brunch: March 31, Chicago, IL
- Collaboration with the Schweitzer Fellowship: ongoing, email Bernice Man for details
- Networking/Educational Dinner Program: Winter 2017, TBD
If you would like to become more involved in the NPN, consider joining our e-board. The time commitment is minimal, but the opportunities are endless! We have monthly, hour long conference calls and encourage participation in at least one other ICHP Committee or Division. Email Bernice.man@uchospitals.edu for more information!
With Gratitude,
Colleen Bohnenkamp, PharmD, BCPS, BCOP
NPN Chair 2016-2017
College Connection
University of Illinois at Chicago (Rockford)
Doughnuts and Morning Rounds
College Connection
by Hannah Dalogdog (P2), ICHP President-Elect
I am not a morning person. I am the sort who considers being awake before sunrise a mild form of torture. And yet, once nearly every week during the last two semesters, I voluntarily made myself get up at six in the morning to make it to campus before 7:30AM. I didn't mind, and I wasn’t the only one. It was for a worthy cause after all: morning rounds.
One benefit of the ICHP student organization I enjoy is MrCAT, or Morning rounds: Cases and Therapeutics sessions. ICHP has made the effort to provide more opportunities for students to receive exposure to clinical pharmacy and one activity is the clinician-led MrCAT, where participants get to dissect real case studies that presenters have encountered in their practice.
MrCAT provides an opportunity for students, like myself, to practice our clinical decision-making skills in a low-stress environment. We use what we have learned in the classroom and apply it to actual patient care scenarios. The patient cases vary and are generally centered on 1 or 2 disease states. Presenters walk student members through the therapeutic process, while providing additional information to supplement the presentation. This way, students from all levels of training can benefit from the discussion. MrCAT not only fosters active learning, but demonstrates how members of a healthcare team could function and why it is crucial to consider everyone's opinions. For an hour each week, pharmacy students from all levels brainstorm patient cases to arrive at the most appropriate therapeutic recommendation. No one is too inexperienced to offer some perspective or seek clarification. For many, this is their first introduction to how a patient care team operates.
With this new academic year comes a new set of weekly, early morning MrCAT sessions to alternate with Journal Club presentations. We are hopeful they will continue to provide another avenue to engage students in conversations centered on therapeutic decision making and direct patient care. Our future goal is to invite practitioners from a variety of clinical practice areas to offer students insight into their unique clinical experiences.
So, at least for now, I let myself enjoy that extra hour of sleep. In less than a month we will begin the bimonthly rounds. I am fortunate to serve on this year's ICHP E-board and I am looking forward to the morning sessions. The doughnuts aren’t half bad either.
SIUE School of Pharmacy
Meet the Board
College Connection
by James Reimer, P-2 and President-Elect
Let
us all say welcome to our new executive board. We are all excited to start a
new school year and get involved in SSHP again!
President:
Kaylee Poole is a P3 who previously
served as our President-Elect and P1 liaison in previous years. She did an
excellent job last year assisting the Executive Board and we are excited to see
what direction she leads us in this year. Kaylee was also appointed as a member
of the ASHP Leadership Development Advisory Group for this year!
Fun fact: Kaylee’s name is a combination of her parents’ middles names—her mom’s middle name is Kay and her dad’s middle name is Lee!
President-Elect:
James Reimer is a P2 who previously
served as the P1 liaison last year. He did a great job promoting P1 involvement
in SSHP last year, and he is excited to continue serving our organization.
James was also appointed as a member of the ASHP Policy and Legislative
Advocacy Advisory Group for this year!
Fun fact: James and his two siblings were all born in different states! (California, Oklahoma, and Illinois)
Vice President:
Abbey Rodeghiero is a P3 who was our
Membership Chair last year. She came to us with many great ideas to encourage
membership, and we cannot wait to see what else she has up her sleeve in her
new role.
Fun fact: Abbey has a crazy obsession with pugs!
Secretary:
Erin Lindstrom is a P3 and was our
Secretary last year. She will continue to use her passion for organization to
help our organization succeed!
Fun fact: Erin has seven siblings!
Treasurer:
Nicole Wheeler is a P3 who previous
served as our ASHP Liaison. We are excited for her to step into this new role
and to keep us fiscally responsible.
Fun fact: Nicole once sold a homemade pie for $550!
Fundraising Chair:
Paris Smith is a P2 and is our new Fundraising
Chair. She is ready to give SSHP her all and learn as much as she can from the
organization and her peers.
Fun fact: Paris has actually traveled to Paris, France as well as two other provinces in France!
Membership Chair:
Kyleigh Maday is a P2 and is our new
Membership Chair. She is ready to use her previous experiences to promote and
increase our membership over last year.
Fun fact: Kyleigh has a new puppy, and her name is Bentley!
Professional Practice
Chair:
Aaron Morris is
a P3 and continuing his role in this position from last year. He did an
excellent job helping inform other students of what their options are after
they graduate, and we look forward to him continuing that this year.
Fun fact: Aaron can count past 20 in four different languages!
Community Chair:
Taylor Hutchison is a P3 is excited to keep
us actively involved in our chapter’s outreach program. She was the Community
Chair last year and did great at organizing our Ronald McDonald House
volunteering.
Fun fact: In her spare time, Taylor likes to bake and decorate cakes for special occasions—including her own wedding!
ICHP Liaison:
Vincent Chau is a P2 looking forward to
all of the opportunities available in this organization. He is looking to
increase his leadership experience as well as being an asset to our
organization.
Fun fact: In Vincent’s free time, his hobby is the sport of boxing!
ASHP Liaison:
Blake Lutzow is a P2 who is excited to
facilitate communication between SSHP and ASHP. He is eager to work with his
peers and strengthen our organization with new ideas.
Fun fact: Blake’s hobby is to play golf, and he has traveled to many different states to play specific courses!
More
Officers and Board of Directors
Executive Officers
 Travis Hunerdosse
Travis Hunerdosse
President
(312) 926-6124
thunerdo@nm.org
 Charlene Hope
Charlene Hope
Immediate Past President
(708) 783-5933
chope@macneal.com
![]() TBD
TBD
President-Elect
 Kathryn Schultz
Kathryn Schultz
Treasurer
(312) 926-6961
kathryn_schultz@rush.edu
 Jennifer Arnoldi
Jennifer Arnoldi Scott Meyers
Scott MeyersRegional Directors
 Amy Boblitt
Amy Boblitt
Regional Director Central
(217) 788-3015
boblitt.amy@mhsil.com
 Elise Wozniak
Elise Wozniak
Regional Director Northern
elise.m.wozniak@gmail.com
 Lynn Fromm
Lynn Fromm
Regional Director
Southern
(618) 391-5539
fromml@andersonhospital.org
Division Directors
 Mary Lee
Mary Lee
Organizational Affairs Director
(630) 515-7311
mleexx@midwestern.edu
 Karin Terry
Karin Terry
Professional Affairs Director
(309) 655-3390
Karin.l.terry@osfhealthcare.org
 Lara Ellinger
Lara Ellinger
Educational Affairs Director
(312) 926-3571
laelling@nm.org
 Carrie Vogler
Carrie Vogler
Marketing Affairs Director
(217) 545-5394
cvogler@siue.edu
 Christopher Crank
Christopher CrankTechnician Representative
 Clara Gary
Clara GaryNetwork and Committee Chairs - non-voting
 Bernice Man
Bernice Man
Chairman, New Practitioners Network
(773) 702-9641
bernice.man.pharmd@gmail.com
 Bryan
Bryan
McCarthy, Jr.
Ambulatory Care Network Co-Chair
773-702-1030
Bryan.McCarthy@uchospitals.edu
![]() Ginny Nash
Ginny Nash
Ambulatory Care Network Co-Chair
 David Tjhio
David Tjhio
Chairman, Committee on Technology
(816) 885-4649
david.tjhio@cerner.com
 Jennifer Phillips
Jennifer Phillips
Editor & Chairman KeePosted
Committee Chair,
Nominations Committee
(630) 515-7167
jphillips@midwestern.edu
 Milena McLaughlin
Milena McLaughlin
Assistant Editor, KeePosted News Journal
(312) 926-4454
milena.pharmd@gmail.com
Student Chapter Presidents
Ashley Shinnick - Chicago State University College of Pharmacy
Maggie Lau - Midwestern University Chicago College of Pharmacy
Kimberly Zaleski - Roosevelt University College of Pharmacy
Aprille Banchoencharoensuk - Rosalind Franklin University
College
of Pharmacy
aprille.banchoencharoensuk@my.rfums.org
Kaylee Poole - Southern Illinois University Edwardsville School of Pharmacy
David Silva - University of Illinois at Chicago College of Pharmacy
ICHP Affiliates
Northern Illinois Society (NISHP)
Erika Hellenbart
President
Denise Kolanczyk
President-elect
Kathryn Schultz
Immediate Past President
David Martin
Treasurer
Milena McLaughin
Secretary
(312) 926-4454
Vera Kalin
Technician Representative
West Central Society of Health-System Pharmacists (WSHP
Ed Rainville
President
ed.c.rainville@osfhealthcare.org
Metro East Society (MESHP)
Jared Sheley
President
Sangamiss Society of Heath-System Pharmacists
Julie Downen
President
217) 788-3953
Katelyn Conklen
Immediate Past President
Vacant Roles at Affiliates; President, Rock Valley Society;
Southern IL Society; Sugar Creek Society
Welcome New Members!
| New Member | Recruiter |
| Mohammed Abba | |
| Lourdes Abdallah | Gayle Cole |
| Deya Abdeljaber | Shereen Salama |
| Serene Abuzir | |
| Pedro Agredano Jr | Clara Gary |
| Asadullah Ahmadi | |
| Tyler Alverson | Noelle Chapman |
| Makynzie Ashbaugh | |
| Josiah Baker | Henry Okoroike |
| Samantha Bastow | |
| Ani Bekelian | |
| Hagop Bekelian | |
| Rohit Bhonagiri | Linda Fred |
| Patrycja Bidzinski | |
| Beata Bigos | Ashley |
| Michael Billett | |
| Brandon Bontes | |
| Jovan Borjan | Andy Donnelly |
| Jane Bourgerie | |
| Benjamin Bowar | |
| Marisa Brizzi | Andy Donnelly |
| Devon Burhoe | Andy Donnelly |
| David Butler | Andy Donnelly |
| Xuan Cai | |
| Deanne Ruth Capinpin | |
| Cecilia Carter | Rita Edwards |
| Shakita Carter | |
| Tiffany Chairudin | |
| James Chang | |
| Heather Chapman | |
| Michelle Cho | |
| Athena Chukwu | |
| Cassandra Clermont | |
| Nicole Coglianese | Andy Donnelly |
| Lauren Cope | |
| Kaitlyn Craddock | Andy Donnelly |
| Matthew Dandino | |
| Kayla Deacon | |
| Lisa Do | |
| Centrella Dunbar | Annexica Buford |
| Chike Egbuna | Bryan McCarthy |
| Joelle Farano | Megan Corsi |
| David Felts | |
| Melika Fini | Andy Donnelly |
| Angelina Finn | |
| Rachael Fleagle Miller | |
| Yan Gao | |
| Lejla Garic | |
| Tarah Gayotin | Elba Sertuche |
| Mathew Gimbar | Andy Donnelly |
| Deborah Gisi | |
| Nahreen Gulias | |
| Hayden Hagemann | Kimberly Zaleski |
| Amber Hanson | Tory Gunderson |
| Katolina Harkabuz | |
| Meymun Hassan | |
| Mickey Hathuc | |
| Chris Hayek | |
| Erin Hermes | |
| Sohee Im | |
| Jessy Johnson | Margie Villarreal |
| Kelsey Johnson | |
| Betty Joseph | |
| Tina Kakish | |
| Mary Kaneaster | |
| Thomas Karakosta | |
| Sali Kathaua | |
| Amanda Kelly | |
| Karen Khalil | Andy Donnelly |
| Irum Khan | |
| Talha Khan | |
| Stephanie Khin | |
| Tiffany Kiehna | Anna Stewart |
| Amanda Koja | |
| Jessica Kulawiak | |
| Mary Lacy | Andy Donnelly |
| Alissa Lee | |
| LaNesha Lee | Theophilus Simon |
| Michelle Lee | |
| Michelle Sunwoo Lee | |
| Charlyn Leon | Shivek Kashyup |
| Jaymi Lyons | Phillip Connelley |
| Nnebuhe Maraizu | |
| Judy Mathew | |
| Troy McMullen | Linda Fred |
| Jason Mei | |
| Jaclynne Metayer | Andy Donnelly |
| Patrick Mirzakhanian | |
| Arturo Montero | |
| Jessica Mourani | |
| Robin Muhammad | |
| Matthew Mulvaney | |
| Kathryn Mundi | Andy Donnelly |
| Danielle Murphy | |
| Oriana Napoleun | |
| Patrick Ndungu | Vicelle Sibal |
| Hue Nhan | |
| Taofikat Olawale | |
| Gretchen Olson | |
| Russell Orr | |
| Tara Ostrander | |
| Jeffin Panickar | |
| Ye Larm Park | |
| Jaini Patel | Jill Borchert |
| Ravi Patel | |
| Lauren Pratt | |
| Samah Qusmieh | |
| Summer Record | |
| Jessica Regan | Margie Filpi |
| Alyse Rehberger | Kelly Moran |
| Annika Richmond | Linda Fred |
| Alice Robertson-Smith | |
| Niveen Salah | |
| Veronica Salgado | Antoinette Cintron |
| Zachary Samples | |
| Jessica Schlotfeldt | |
| Meliton Sedano, Jr. | |
| Pooja Shah | |
| Michael Shaw | |
| Munir Shukla | |
| Kamila Sibiga | |
| Samantha Socco | |
| Erin St. Angelo | |
| Meagan Sullivan | |
| Ashish Suthar | |
| Christopher Swims Vernor | |
| Khushbu Tejani | Andy Donnelly |
| Jessica Thomas | |
| Rachel Thomas | |
| Le Tran | |
| Elaine Trinh | |
| Hannah Underwood | Andy Donnelly |
| Lindsey Veitch | |
| Gwen Volpe | |
| Phi Vong | |
| Amy Wainright | |
| Jill Waldhoff | Mandy Davis |
| Ashley Walter | Amy Maxfield |
| Jamila Watkins | Linda Fred |
| Samantha Wiesinger | |
| Karolina Wojciak | |
| Brentsen Wolf | |
| Helen Wondowassen | |
| Paa Kwesi Yahful | Andy Donnelly |
| Sanja Zepcan |
ICHP Pharmacy Action Fund (PAC) Contributors
Upcoming Events
Visit the ICHP Calendar for the most up-to-date events! 
Saturday, October 7, 2017 - Carterville, IL
American Heart Association - Heart Walk
Tuesday, October 10, 2017 - 6:00 PM
Addressing the Time Crunch: Making the Relationship Mutually Beneficial for the Site, Preceptor and Student
Alison Stevens, PharmD, BCPS
Sangamiss LIVE Program
Lake Pointe Grill
1386 Toronto Road, Springfiled, IL 62712
5:00 pm Registration
6:00 pm Program
7:00 pm Dinner
Accredited for pharmacists |1.0 contact hour (0.1 CEU)
Thursday, October 12, 2017 - 6:00 PM
Biologics and Biosimilars: From Bench to Bedside
Alexandra Terry, PharmD
West Central LIVE Program
Proctor Hospital, Proctor Private Dining Room
Peoria, IL
Accredited for pharmacists and pharmacy technicians |1.0 contact hour (0.1 CEU)
Watch for more information in upcoming news briefs.
Thursday, October 19, 2017 - 6:00 PM
On the Horizon and in your Backyard: Updates in Infectious Diseases
Thomas D. Chiampas, PharmD, BCPS, AAHIVP
Jessica M. Cottreau, PharmD
NISHP LIVE Program
Accredited for pharmacists and pharmacy technicians |1.25 contact hour (0.125 CEU)
Tuesday, November 7, 2017 - 12:00 PM
Probiotics: Their Role in Medicine Today
Viktorija Barr, PharmD
Champions LIVE Webinar
Accredited for pharmacists and pharmacy technicians |0.5 contact hour (0.05 CEU)
Tuesday, November 14, 2017 - SAVE THE DATE
How low should we go: Evaluating Targeted Temperature Management and Its Use in Clinical Practice
Dalena Vo, PharmD
Sangamiss LIVE Program
Pao Bistro
2824 Plaza Drive, Springfield, IL 62704
Save the date! Watch for more information in upcoming news briefs.
Wednesday, January 17, 2018 - SAVE THE DATE
NSAIDs and MI
Elizabeth Van Dril, PharmD
Champions LIVE Webinar
Save the date! Watch for more information in upcoming news briefs.
