Print Entire Issue

KeePosted Info
Columns
President's Message
Directly Speaking
New Practitioners Network
Leadership Profile
Government Affairs Report
Educational Affairs
ICHPeople
College Connections
Rosalind Franklin University College of Pharmacy
Midwestern University Chicago College of Pharmacy
Roosevelt University College of Pharmacy
More
Welcome New Members!
Officers and Board of Directors
ICHP Pharmacy Action Fund (PAC) Contributors
Upcoming Events
KeePosted Info
Illinois Council of Health-System Pharmacists
4055 North Perryville Road
Loves Park, IL 61111-8653
Phone: (815) 227-9292
Fax: (815) 227-9294
ichpnet.org
KeePosted
Official Newsjournal of the Illinois Council of Health-System Pharmacists
EDITOR
Jacob Gettig
ASSISTANT EDITOR
Jennifer Phillips
MANAGING EDITOR
Scott Meyers
ASSISTANT MANAGING EDITOR
Trish Wegner
DESIGN EDITOR
Amanda Wolff
ICHP Staff
EXECUTIVE VICE PRESIDENT
Scott Meyers
VICE PRESIDENT - PROFESSIONAL SERVICES
Trish Wegner
DIRECTOR OF OPERATIONS
Maggie Allen
INFORMATION SPECIALIST
Heidi Sunday
CUSTOMER SERVICE AND
PHARMACY TECH TOPICS™ SPECIALIST
Jo Ann Haley
ACCOUNTANTS
Jan Mark and Trisha Blassage
COMMUNICATIONS MANAGER
Amanda Wolff
LEGISLATIVE CONSULTANT
Jim Owen
ICHP Mission Statement
Advancing Excellence in Pharmacy
ICHP Vision Statement
ICHP dedicates itself to achieving a vision of pharmacy practice where:
- Pharmacists are universally recognized as health care professionals and essential providers of health care services.
- Patients are aware of the training, skills, and abilities of a pharmacist and the fundamental role that pharmacists play in optimizing medication therapy.
- Formally educated, appropriately trained, and PTCB certified pharmacy technicians manage the medication distribution process with appropriate pharmacist oversight.
- Pharmacists improve patient care and medication safety through the development of effective public policies by interacting and collaborating with patients, other health care professionals and their respective professional societies, government agencies, employers and other concerned parties.
- Evidence-based practices are used to achieve safe and effective medication therapies.
- There are an adequate number of qualified pharmacy leaders within the pharmacy profession.
- Pharmacists take primary responsibility for educating pharmacy technicians, pharmacy students, pharmacist peers, other health professionals, and patients about appropriate medication use.
KeePosted Vision
As an integral publication of the Illinois Council of Health-System Pharmacists, the KeePosted newsjournal will reflect its mission and goals. In conjunction with those goals, KeePosted will provide timely information that meets the changing professional and personal needs of Illinois pharmacists and technicians, and maintain high publication standards.
KeePosted is an official publication of, and is copyrighted by, the Illinois Council of Health-System Pharmacists (ICHP). KeePosted is published 10 times a year. ICHP members received KeePosted as a member benefit. All articles published herein represent the opinions of the authors and do not reflect the policy of the ICHP or the authors’ institutions unless specified. Advertising inquiries can be directed to ICHP office at the address listed above. Image disclaimer: The image used in the Pharmacy Tech Topics™ advertisement is the property of © 2016 Thinkstock, a division of Getty Images.
Copyright © 2016, Illinois Council of Health-System Pharmacists. All rights reserved.
Columns
 President's Message
President's Message
Time to Innovate
by Charlene Hope, PharmD, MS, BCPS, ICHP President
I want to thank Immediate Past President, Jen Phillips, for the dedication, passion and enthusiasm that she brings to ICHP. Her contributions are invaluable. I know that over the last year, I found myself instilling her theme and philosophy of “Leadership, It’s Not Just for Leaders!” to the pharmacists that I work with on a daily basis.
From the bottom of my heart, I want to thank each of you for the great honor of serving as the 53rd President of Illinois Council of Health-System Pharmacists. After I first became involved with ICHP as a student leader of the Midwestern University Chicago College of Pharmacy Student Chapter, I don’t think I ever imagined that I would one day serve as President; especially, when at the time the members of the executive board looked nothing like me.
However, it was what I had in common with this dynamic group of men, whose passion and dedication to hospital/ health-system pharmacy practice and whose vision of what ICHP could accomplish in advancing the profession, by promoting the role of the hospital pharmacist that inspired me to become actively involved. Throughout my career, regardless of where I have worked, ICHP gradually became and remains my pharmacy home.
A few memories from over the years came to mind as I was preparing for today’s address. The first time I attended the ICHP student leadership retreat, it was held at the Chicago Botanical Garden and it was also the first time I went to the Ravinia Festival and ate at Ed Debevics. My most favorite memory is, and she probably does not remember this, at one of my first leadership retreats – Ann Jankiewicz showed me this brand new browser called Google and excitedly shared with me how it was way better than Yahoo in finding information on the internet. Last night, Mary Ann Kliethermes and I reminisced over the time that she and Janet Teeters ventured down to Chicago for a planning meeting that I hosted for them in my walk-up apartment when I first moved to the city. And a couple of years ago, right here at the Annual meeting, Mike Fotis shared his words of advice and support as I was contemplating a challenging situation at work. It’s these moments and friendships (old and new) that I have developed over the years that keep me connected and committed to ICHP and its continued success.
Professor Shalowitz’s syllabus was the most interesting one I had read in the long time. The level of detail of the 12-page document accounted for every possible scenario he has probably ever encountered with a student. I remember thinking to myself, if this is his syllabus, passing his class was not going to be a walk in park. Fast forward to the first day of class making sure I was sitting in the first three rows as his syllabus instructed, he introduced himself and started his lecture with slides of the most beautiful pictures of sculptures and paintings and how they related to healthcare. And while the beautiful pictures were soon replaced with charts, graphs and clippings from the media; there was a theme that he had for the course and he continued to repeat throughout. “There is nothing new in healthcare and what is old will become new again.” Remembering this, I decided for this inaugural address I would read some addresses and the themes of the Presidents that came before me spanning about 10 years.
Mike Weaver, in his 2006 presidential address; spoke of the role of technology, legislation and regulations; all of which he stated were going to start to have a major impact on pharmacy and the healthcare industry as a whole and were only going to continue to further expand and involve.
Chris Rivers, in her 2011 presidential address spoke of the complexity of our lives at home and at work and the challenges of fitting all that we want to achieve, personally and professionally, into the limited time that we have over the course of the days and years of our lives.
Avery Spunt and Ann Jankiewicz spoke to themes of staying vigilant and fighting complacency.
The challenges facing us as individual pharmacists, our departments and practices, and the profession as a whole remain the same and over the years with advancing technology and increasing access to data seem to introduce more and more complexity. So, I too, agree with Professor Shalowitz, there is nothing new in healthcare.
In this current era of Healthcare Reform and increasing focus on Healthcare Quality and Safety to the gradual transition in reimbursement models from fee for service to value-based payment, the pressure is on for us, as pharmacists, to start taking greater accountability and focus on connecting the positive impact that we make every day on the outcomes and experiences of our patients; and making the connection to the cost of providing those services. Dr. Manasse, in his general session address yesterday, spoke to this point. Becoming healthcare providers and having our names listed in the Medicare roster is only half the battle. The other is related to reimbursement and defining what our services are and how much those services are deemed to be worth. In today’s healthcare climate, we need to match the level of our clinical expertise with our business acumen and understanding the business of healthcare which also is NOT just for leaders.
Our mission, if you choose to accept it, is to actively participate in redesigning healthcare delivery. Where do pharmacists fit in this new healthcare delivery system and how do we contribute to the value of the healthcare? The challenge still remains on how much we should charge and get reimbursed for our services yet, the opportunities are abundant.
- Hospital Readmissions - $ 41.3 billion opportunity
- Poor Medication Adherence - $290 billion per year opportunity
- Opioid Medication Misuse and Abuse - $72 billion per year opportunity
- Adverse Drug Events - $6 million per hospital opportunity
Not too long ago, ICHP celebrated its 50th anniversary. Take some time to imagine, what actions we will need to take today for ICHP to remain a strong, vibrant, financially strong organization through the next 50 years? The title of a popular leadership book by Marshall Goldsmith comes to my mind – What got you here, won’t get you there. How do we get “there” – working on the numerous opportunities, navigating our challenges and advancing our profession? Through INNOVATION, my presidential theme for this upcoming year.
In the field of patient safety, we often look at industries outside of healthcare and adapt safety practices from those industries and apply them in healthcare. Chicago is the home of numerous healthcare start-up company incubators. Start-up company incubators are a place for new companies full of entrepreneurs to learn the skills to become larger, successful companies. I want to challenge us to adopt three skills of start-up entrepreneurs who live and breathe innovation.
1) Courage.
What’s the biggest impediment to innovation within an organization? Fear. As early as 2004, research from Elizabeth Wolf Morrison and Frances J. Milliken for the Academy of Management Review and Stern Business pegged fear — and the resulting silence when employees operate within a culture of fear — as the biggest roadblock to innovation. So we must take heart and Be Bold as Mike Fotis encouraged us to do in 2013.
2) Adopting “failure” as a synonym for “learning opportunity”.
“Fail fast and fail often” is a common mantra of entrepreneurs. Failure is not a word that we as pharmacists ever want to hear – priding ourselves on asking all possible questions and considering every possible scenario with attention to detail, ensuring that all the i’s are dotted and t’s are crossed before launching a process change or new initiative. But this mantra really serves as a reframing of failure from a personal fault to learning and improving on a continuous basis. With technology and business cycles moving so quickly, our departments and respective organizations no longer have the luxury of waiting a year or more to launch a new service or performance improvement project.
3) Creativity.
Creativity is something we often equate with actors, singers and fashion designers. The truth is we all have the capacity for creativity. Creativity is a function of knowledge, curiosity, imagination, and evaluation. The greater your knowledge base and level of curiosity, the more ideas, patterns, and combinations you can achieve, which then correlate to creating new and innovative products and services. But merely having the knowledge does not guarantee the formation of new patterns. The bits and pieces must be shaken up and iterated in new ways. Then the embryonic ideas must be evaluated and developed into usable ideas. In other words, there really is a process. And who knows processes better than pharmacists?
How many of you have taken an Uber or booked accommodations through Airbnb? What can we learn from these disruptive, innovating companies? Perhaps, I can make the case that we work on disrupting our own industry. To me, no industry (including healthcare) is immune to disruptive innovation. What’s on the horizon?
Drug auto verification of medication orders – while most recent studies revealed pitfalls, remember that technology grows exponentially. Clinical surveillance technology – MedCPU program compiles data from free text and structured fields within your organization’s eHR, interfaced with the hospital formulary, your hospital’s workflows, protocols and best practices (including that of the pharmacy) and identifies gaps in care and provides the prescriber customized therapeutic options in real time.
We have to be able to adapt quickly and collaborate with all members of the team and take the lead in any opportunities or setting where medication management is needed. We cannot afford to wait to be asked to participate in programs that we know would benefit from the expertise of the pharmacist.
This is what I believe…
I believe in the power of diversity.
I believe in the power of our ideas.
I believe in the power of our ability to choose our own destiny.
I invite you, the leaders, staff and members of ICHP to join me on this journey, because ladies and gentlemen, it is time for us to innovate.
Thank You.
 Directly Speaking
Directly Speaking
Attention PTCB Certified Technicians!!!
by Scott A. Meyers, Executive Vice President
If the title of this month’s column got your attention, chances are, you’re a PTCB certified tech or someone who works with one or more of them. And that’s great! Because I want to share some important information that should convince you or them to maintain your or their PTCB certification.
First of all, let me share some facts for certified pharmacy technicians who practice in the once great State of Illinois. While Illinois requires new pharmacy technicians to obtain certification prior to their second license renewal, the State does not limit certification by the Pharmacy Technician Certification Board, Inc. (PTCB) only. The Pharmacy Practice Act requires “he or she has successfully passed an examination accredited by the National Organization of Certifying Agencies, as approved and required by the Board.” Unfortunately, there is another examination available that meets that requirement, although little is known about the test details, and ownership is not by pharmacy professional organizations but rather a for-profit entity. In addition, the State of Illinois does not require that once certified, pharmacy technicians maintain their certification. The State does now require that all certified pharmacy technicians obtain 20 hours of ACPE approved continuing pharmacy education (CPE) every two years including at least one hour of pharmacy law and one hour of patient safety CPE beginning in 2017. By the way, these are the same requirements for maintaining PTCB certification.
Now, let me share the many reasons why every Illinois PTCB certified pharmacy technician should maintain their certification.
- You now have to obtain the same CPE credits in Illinois to maintain your registration as you do to maintain your PTCB certification. The only extra component is the $40 recertification fee. Because Illinois requires ACPE approved technician CPE credits, NABP’s CPE Monitor can and most likely will be used to document compliance. PTCB also uses NABP’s CPE Monitor to verify compliance so reporting will become infinitely more reasonable for both programs.
- What if you want to move to another State? The Pharmacy Technician Certification Examination (PTCE) is administered in all 50 States, and 23 of those States and the District of Columbia include the PTCE in their regulations. If you move to one of those States, you will need to maintain your certification! Or take the test again, which seems to me like a much bigger challenge. But it is your call.
- What if you want to change employers? While PTCB certification is not a State requirement, it is a requirement of many Illinois hospital pharmacy directors. You may not have to have already passed the PTCE to work in one of these hospitals, but you may be required to pass it within a certain amount of time on the job. So why wouldn’t you be better off maintaining your initial certification rather than have to take the test again, or worse yet, lose out on a great job opportunity because you let your certification lapse! I promise you, I will never let my Illinois pharmacist license lapse until I can no longer think of working in a pharmacy, even though ICHP doesn’t require me to keep mine active.
- PTCB is now in the process of developing three new Advance Certifications for Pharmacy Technicians in the areas of Sterile Compounding, Community Pharmacy Practice and Hospital Pharmacy Practice. In every case, current certification by PTCB will be a prerequisite for sitting for these advanced certifications. If you can’t wait for one of these specialty recognitions, you had better have the initial certification intact and up to date!
- Every time you recertify with PTCB, you receive another certificate! While this may be a less significant reason to recertify, those certificates look pretty impressive on the walls of pharmacies across the State, and earlier versions can look very inspiring on an office wall at work or at home. Each new certificate not only represents your current status as a PTCB Certified Pharmacy Technician, but it also represents your commitment to continue to learn and grow because of the minimum 20 hours of CPE credit you had obtained in order to receive each certificate. These certificates represent bookmarks in your life story, and you should be proud to display them.
- Finally, while recertification is not currently a State requirement here in Illinois, it is in some other States, so maintaining your certification now gives you peace of mind just in case the laws ever change here in Illinois and recertification becomes a requirement.
I think I have identified enough reasons why you should maintain your PTCB certification, even though it is not currently required in Illinois. I know I sure would if I was a PTCB CPhT! Yes, the $40 every two years is money you might not need to spend, but someday or at some job it might be and that $40 looks a lot easier to come up with than retaking the PTCE, missing out on a sweet job, or changing careers because you have to move to another state.
If you agree, make sure you recertify and make sure you share this with your PTCB certified colleagues. They will appreciate it and hopefully you have, too!
New Practitioners Network
Team ICHP raises over $500 for the Juvenile Diabetes Research Fund and Walks to Cure Type 1 Diabetes
by Colleen Bohnenkamp, PharmD, BCOP, BCPS
 The Juvenile Diabetes Research Fund (JDRF) One Walk was held on Sunday, October 3rd at Montrose Harbor in Chicago. It was the 3rd year Team ICHP has participated in the walk, and our team raised $505 to benefit Type 1 Diabetes (T1D) Research in the pursuit of creating, “A World without Type 1 Diabetes.”
The Juvenile Diabetes Research Fund (JDRF) One Walk was held on Sunday, October 3rd at Montrose Harbor in Chicago. It was the 3rd year Team ICHP has participated in the walk, and our team raised $505 to benefit Type 1 Diabetes (T1D) Research in the pursuit of creating, “A World without Type 1 Diabetes.”
The morning began with live music and several welcome activities. Vendor booths offered samples of products for patients with Type 1 Diabetes, such low glycemic bars. The opening ceremony was kicked off with a warm-up from Pure Barre©, followed by the singing of the National Anthem, and a short speech from Ron Santo, Jr., who spoke of how his late father had two wishes in life - a cure for T1D, and for the Cubs to win the World Series. Looks like one of his wishes has become a reality this year!
My husband, who does not work in healthcare, joined me on the walk this year as I was 9 months pregnant. Before we began, he shyly asked me, “What is Type 1 Diabetes”? While I giggled and was surprised he wasn’t aware of the disease, it occurred to me that the majority of the population probably is unaware of the implications of T1D. In fact, I’m sure many families with children suffering from T1D had little to no prior knowledge of the disease and the lifetime commitment it entails prior to diagnosis.
I explained to my husband that T1D is an autoimmune disease where the pancreas stops producing insulin. It most commonly presents in childhood and has nothing to do with diet or lifestyle. It results in families and young children being forced to learn how to count carbohydrates and poke themselves several times per day to check their blood sugar and administer insulin. In addition, close monitoring of the types and amounts of food they can eat and their activity levels is required. There can also be considerable anxiety about the potential complications of low blood sugar, such as seizures. Add the potential of several long term health complications, such as heart and kidney disease, and it starts to become clear what an onerous disease this is.
With our own child arriving in a few short weeks, I think my husband really began to understand how challenging and burdensome this disease can be, and how finding a cure should not simply be a wish, but needs to be a reality! Although I suppose I should not have giggled too much about his lack of T1D knowledge, as I had to embarrassingly ask him, “Who is Ron Santo”?
As we walked along the beautiful lakefront trail, two things were apparent: the power of community and the support it provides to T1D sufferers. The walkers who suffered from T1D proudly wore bandanas, signifying their daily reminder of what it means to live with this disease. Several also wore distinct shirts or apparel to differentiate themselves from their supporters. As we walked together, the presence of a unified community coming together to support each other and achieve a common goal of raising funds to stomp out T1D was inspiring. Together, the Chicago walkers raised a total of $939,547.21!
The race concluded with lunch from Buona Beef, live music, face painting, and entertainment from the Jesse White tumblers. As in previous years, Project S.N.A.P. was on site to turn our individual art pieces into a collective mosaic that will be completed and available for online viewing beginning in December at projectsnap.org. While Team ICHP did not have as many walkers as in previous years, I am so proud that we continue to support such an important cause and seek opportunities to make an impact in the lives of others.
On behalf of Team ICHP, I want to sincerely thank everyone who donated to support our team or who joined us on the walk this year. The Chicago walk was just one of more than 200 One Walk locations across the country. If you are interested in learning more about T1D research, participating in a walk near you, or would like to make a donation to the JDRF, visit www.jdrf.org/walktocure.
Ron Santo’s dreams have come true! No more next years! #FlyTheW #AWorldWithoutT1D
EDITOR'S NOTE: Since completion of this article, author, Colleen Bohnenkamp, has given birth to a healthy baby boy! See sweet Theo in the November ICHPeople.
Leadership Profile
Denise M. Kolanczyk, PharmD, BCPS, AQ-Cardiology
 What is your current leadership position in ICHP?
What is your current leadership position in ICHP?I am currently one of the members of the Marketing Affairs Division.
Where did you go to pharmacy school?
I attended Butler University College of Pharmacy and Health Sciences in Indianapolis, IN.
Trace your professional history since graduation. Where have you trained / worked, any special accomplishments?
Upon graduating in 2009, I began a 2-year Pharmacotherapy Residency at Indiana University Health in Indianapolis, IN. It was also affiliated with Butler University. I received training focused in internal medicine, ambulatory care, and academia. It was the first big step that aided in my development of being a clinical pharmacist and educator.
My first position was a Clinical Pharmacy Specialist in Cardiology at The University of Chicago Medicine. In addition to my patient care responsibilities, I precepted pharmacy students from Chicago State University and the University of Illinois-Chicago on medicine/cardiology APPE rotations. I also was heavily involved with our pharmacy residency programs, and later became the residency program director for the PGY2 Cardiology Residency program.
Describe your current area of practice and practice setting.
I obtained a position with Midwestern University Chicago College of Pharmacy with a practice site at Loyola University Medical Center in the fall of 2014 that aligned well with my career goals. I spend 50% of my time on campus which is dedicated towards teaching, service, and scholarship. I spend the remaining 50% practicing as a clinical pharmacist in internal medicine at my practice site, and round with a general medicine team daily. I precept both IPPE and APPE students. I also precept 1 or 2 PGY1 pharmacy practice residents at Loyola University Medicine Center on their general medicine rotation.
What initially motivated you to get involved, and what benefits do you see in being active in a professional association such as ICHP?
During my time as a resident in Indiana, I was a member of a state level, professional pharmacy organization. I was the resident liaison and worked closely with the chapter officers. I enjoyed networking with others throughout the state and the volunteer opportunities. It also taught me the value of getting involved outside your institution and how that can aid in your professional growth and development.
ICHP offers a lot of different opportunities for professionals to get involved. I think it’s great we have a specific network devoted to new practitioners. It’s a great resource for new pharmacy graduates, especially those from out-of-state coming to practice here, to show them what ICHP is all about and the ways to get involved.
Is there an individual you admire or look up to, or a mentor that has influenced your career?
It is challenging to pick just one mentor as I have a few that I call upon or walk down the hall to talk to. During my second professional year at Butler University, I began to realize my strong interest for clinical pharmacy. Dr. Alexander Ansara (Butler University/Indiana University Health) was one of the first professors I had who opened my eyes to the world of both clinical pharmacy and academia. Throughout my advanced pharmacy practice experiences and residency, I also developed a strong interest in student precepting and teaching. Initially, I wanted to be a teacher when I was younger, and I was intrigued that you could do both as a pharmacist. Dr. Ansara later became my APPE preceptor for general medicine, residency project mentor, and PGY2 internal medicine/cardiology preceptor. I have modeled approaches to student lectures, topic discussions, and clinical practice based on observations and feedback I received from him. We still keep in touch, and recently collaborated on a publication together.
Do you have any special interests or hobbies outside of work?
I enjoy traveling to new places each year. I visited Hawaii and Arizona for the first time in 2016. I’m in the process of planning a trip to Germany, France, and possibly Austria for next fall. I like watching sports, and am a big baseball fan (Go White Sox!). If able, I enjoy visiting stadiums that I haven’t caught a game at while I’m traveling. I was able to visit two this past season: Chase Field in Phoenix, AZ and Target Field in Minneapolis, MN. When I’m home in the city, I enjoy trying new recipes. I’ve been able to enhance my culinary skills and recipe bank over the past several years.
Do you have a favorite restaurant or food?
My go-to favorite is Osteria La Madia in the River North neighborhood of Chicago. In addition to their wood-fired pizzas, they have the best oven-roasted artichokes I’ve ever tasted.
What 3 adjectives would people use to best describe you?
Happy, caring, ambitious.
Government Affairs Report
Senator Karen McConnaughay’s 2nd Annual Women’s Conference
by Guest Columnist - Cheryl Lynn Hayes, PharmD, MBA, MJ, BCPS
I was eager and willing to represent the Illinois Council of Health-System Pharmacists once again at the 2nd Annual Women’s Conference sponsored by Senator McConnaughay and held at Elgin Community College on October 6th. While rushing (and possibly speeding) to arrive to the event on time after finishing work, I was slightly delayed by two of Elgin’s finest men in blue (i.e. police). However, upon mention of my destination, I was spared the speeding ticket and encouraged to enjoy the Senator’s event and to be observant of posted speed limits.
During Senator McConnaughay’s opening remarks, she graciously acknowledged the many women mentors and role models who influenced and supported her career throughout the years. In efforts to promote collegiality and networking among women, the Senator developed this forum with hopes to facilitate similar connections and influence among Illinois women. Everyone in attendance had an opportunity to provide a brief “biography”; the audience included women representing many sectors of our business economy, including health, education, banking, engineering, manufacturing, public policy, government, social services, etc.
With the theme of “Educate, Empower, and Engage,” the agenda provided opportunities to learn from the challenges and experience of several women leaders in business, social service, advocacy and engineering disciplines. The keynote speaker was Dr. Beth Purvis, Illinois Secretary of Education, who serves in the administration of Governor Bruce Rauner. She spoke openly and candidly about her career path, current responsibilities and relationship with the Governor. This was followed by a panel discussion of three distinguished women, who spoke of their greatest challenges, rewards, and invaluable mentor relationships that provided guidance when crucial decisions had to be made. These panelists were Gloria Bunce, Director of CASA Kane County, Catherine Tojaga, President of CT Mechanical, and Gretchen Vapnar, Executive Director of the Community Crisis Center, Inc. in Elgin, Illinois.
It was a privilege to represent ICHP and the pharmacy profession at this meeting. Thanks to Scott for inviting me to participate. The following video highlights the mission of this year’s Women’s Conference (I was caught on film at the 1:28 mark! I’m the blond woman with the black jacket. Unfortunately, you only catch my back.): https://www.youtube.com/watch?v=a2USnWc_mKE&feature=youtu.be
EDITOR'S NOTE: This is a great example of how any ICHP member can get involved in their legislative district and carry pharmacy’s voice to legislators around Illinois. We encourage any ICHP member that gets involved in their districts to report special activities to us so that we may share and highlight them with the entire membership. Thank you, Cheryl, for stepping up!
Educational Affairs
Impact of Patient Health Literacy on Pharmacists’ Workload in an Ambulatory Care Setting
by Renee Papageorgiou, PharmD, Clinical Pharmacy Specialist, NorthShore University HealthSystem, Glenview, IL; Jill Borchert, PharmD, BCACP, BCPS, FCCP, Professor and Vice Chair, Pharmacy Practice, Midwestern University Chicago College of Pharmacy, Downers Grove, IL; Mary Ann Kliethermes, BS, PharmD, Professor and Vice Chair, Pharmacy Practice, Midwestern University Chicago College of Pharmacy, Downers Grove, IL
Introduction:
The National Library of Medicine defines health literacy as “the degree to which individuals have the capacity to obtain, process, and understand basic health information and services needed to make appropriate health decisions.”1 Due to the complexity of health terminology and documents, approximately 90 million people have difficulty understanding health-related information. Many components make up literacy including print literacy, oral literacy, numeracy and conceptual knowledge.2 Given the complexity of literacy, an individual may successfully communicate on a daily basis, but may not be able to apply the same skills in a health-related setting. Health literacy is impacted by factors such as age, income, and ethnicity.1
Health literacy plays a role in many situations including the need to consent to a procedure, understand test results, participate in encounters with healthcare professionals, and properly take a medication.1,2,3 While there is no specific definition of adequate versus low health literacy, the National Work Group on Literacy and Health recommend verbal and written communication of health information occur at a fifth-grade level or less.4
Emphasis is currently being placed on self-management of one’s health. This can be difficult for individuals with low health literacy since understanding health information is not just related to being able to read documents, but to understand the material, analyze it and make a decision based on the provided information.3 Roughly 12% of adults have proficient health literacy, necessary to accurately interpret a prescription label.5 Incorrectly reading a prescription label can lead to a higher medication error rate and/or medication non-adherence, resulting in poor health outcomes, increased hospitalizations and/or mortality. Hospitalizations due to poor drug adherence cost approximately $100 billion per year.5,6
One study evaluating written and verbal communication with patients in various outpatient pharmacy settings suggested that medical jargon is often used and pharmacists need improvement when communicating with patients.7 Healthy People 2020, an initiative that sets up healthcare improvement goals every ten years, is currently focusing on health literacy and how to improve patient-healthcare professional communication.8 Pharmacists in community and clinic-based practices are easily accessible to patients and can provide care for patients of all literacy levels.4 Pharmacists can provide services including, but not limited to, administering health literacy assessments or preparing individual pill cards for patients to assist in proper medication administration.9 Pharmacists can also play a role in reducing health literacy related costs by providing assistance to patients with both proficient and low health literacy, which can help to prevent health literacy-related consequences.
The effect of health literacy on pharmacists’ workload is unknown. Depending on the area of practice, workload may include identifying drug-related problems during a clinic visit, ordering patient labs, or filling prescriptions. Past studies evaluated how varying health disparities affect pharmacists’ workload in pharmacist-managed anticoagulation clinics. A study conducted by Meade and colleagues focused on health disparities such as gender, race, education, and income, but did not address health literacy.10 The study was conducted at two clinics in the Chicagoland area with heterogeneous patient populations. It showed an 8.4 minute increase in pharmacist time needed to provide care in a clinic serving an underserved, minority population compared to a clinic providing care to Medicare and supplemental insured individuals at high risk for multiple disease state complications and frequent hospitalizations.10 There are currently no formal studies published regarding the relationship between patient health literacy level and pharmacists’ workload and/or required patient visit times.
Objectives:
The primary objective of this study was to discover whether the degree of patient health literacy affected a pharmacists’ workload during a single clinic visit. The secondary objective of this study was to determine if there was a difference in time spent completing various pharmacist-related tasks during a clinic visit between health literacy groups.
Methods:
Prior to implementation, this study was reviewed and approved by the Institutional Review Boards at Advocate Health Care and Midwestern University. The study was conducted at the Advocate Medical Group Beverly Center, located in a southwestern neighborhood of Chicago. This pharmacist-run clinic is part of a physician-led medical group within an ambulatory care division of a large healthcare system. The clinic serves primarily an insured, urban, minority population five days per week. Services provided by the clinical pharmacists include anticoagulation management, and chronic disease management (CDM) for diabetes, hypertension, and dyslipidemia. Initial and follow-up anticoagulation clinic (ACC) visits are scheduled for 30 and 15 minutes, respectively. Sixty-minute visits are reserved for initial CDM visits, and 30 minutes for follow-up CDM visits. Pharmacy students completing their advanced pharmacy practice experiences at the clinic also participate in ACC and CDM visits.
The study was conducted one to three days per week for 6 weeks from April through June 2015. This cross-sectional, pilot study was completed in two parts. Part one of the study involved collecting patient demographics and having the patient complete the Short Assessment of Health Literacy – English Version (SAHL-E) assessment prior to the clinic visit. This instrument was selected because it is a validated health literacy assessment used to identify patients as being adequate or low health literate.11 During the second part of the study, the research investigator (PGY1 Pharmacy Practice Resident) or a trained research assistant (pharmacy student) observed the patient visit and recorded the total time spent for the clinic visit and also the time spent on numerous activities completed by the clinical pharmacist or the pharmacy student.
The primary study outcome was to determine if the patient’s health literacy level affected the length of a single clinic visit. Patients were eligible to participate if they were scheduled for an appointment with the clinical pharmacist on a study day and if they met the following inclusion criteria: English-speaking adults 18 years and older, able to fill out the demographic questionnaire, able to respond to the SAHL-E assessment. Patients were excluded if they were non-English speaking, diagnosed with a cognitive impairment, had a diagnosis of aphasia or deafness, reported they were unable to read English, and/or were unable to give informed consent. Patients returning for a follow-up visit within the study period were only eligible to participate once, and were excluded from any subsequent observations.
Prior to starting the clinic visit and following consent, the demographic questionnaire was administered. The questionnaire contained questions related to the patient’s age, ethnicity, education level, estimated income, gender, health care coverage, primary spoken and written language, and if the patient required assistance from a caregiver or family member. After the questionnaire was completed, the patient completed the 18-item SAHL-E assessment. Each notecard had a stem word on line one and two additional words on the second line (one key word and one distractor word). The patient would read the stem word out loud, and an investigator or research assistant would ask, “Which word is associated to the stem word?” Missing four or more associations (SAHL-E score ≤ 14) would result in identifying the patient as having inadequate health literacy. To prevent upsetting the patient or causing them any unforeseen harm, the assessment was stopped after the subject missed four associations, even if all 18 words were not tested.
Following the SAHL-E assessment, the clinical pharmacist or pharmacy student entered the room to conduct the clinic visit. During this time, the research investigator or assistant remained in the room and observed the visit. Using a stopwatch, the research investigator or assistant recorded (on a self-designed data collection tool) the length of the clinic visit, and the total number of minutes spent on various tasks completed during the visit including, but not limited to: comprehensive medication review, identification of drug-related problems and/or non-adherence, patient interview, plan development, drug therapy recommendation, and/or patient education. In additional to the total clinic visit time, any time spent completing tasks related to the patient following the clinic visit (writing patient note, ordering refills, ordering labs) was also recorded. Any work that continued to another day was not captured.
Study data were collected and managed using REDCap (Research Electronic Data Capture), a secure, web-based, electronic data capture tool hosted at Midwestern University.12
The student t-test was used to compare total pharmacist/student pharmacist visit time between patients with adequate health literacy and low health literacy. Descriptive statistics were used to summarize total visit time, patient demographics, SAHL-E results, and the amount of time spent on various tasks during the clinic visit. All results are reported using minutes, frequencies, and percentages. Analyses were performed using SPSS (PASW Statistics 19, SPSS Inc., Chicago, IL).
Results:
A total of three clinical pharmacists and three pharmacy students were observed during the study period. The pharmacists had the following certifications: Board Certified Pharmacotherapy Specialist® (n=1), Board Certified Ambulatory Care Pharmacist® (n=2), and Certified Anticoagulation Care Pharmacist (n=1). The majority of the visits were conducted by a clinical pharmacist (n=34, 81.0%) with the remainder conducted by a pharmacy student (n=8, 19.0%).
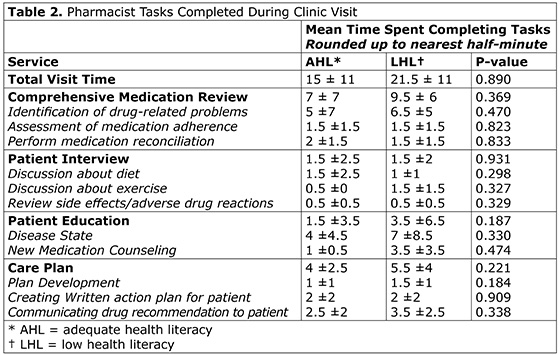
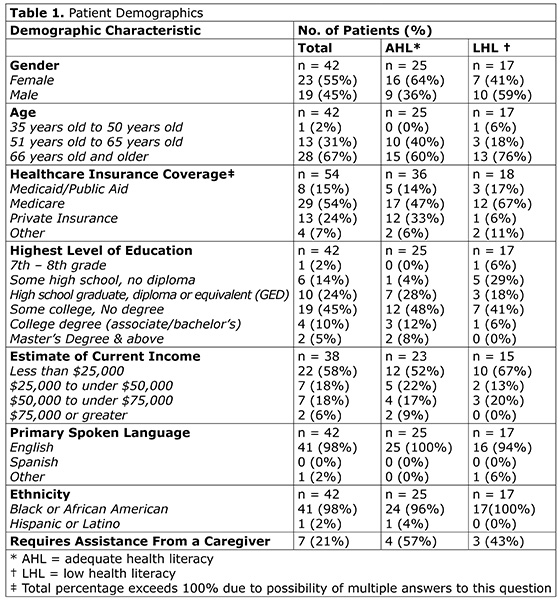
During the study period, 78 patients were eligible to participate in the study. All patients who consented to the study were included in the analysis. Fifteen patients did not consent, and 21 were excluded. Thirty-eight percent (n=8) of patients were excluded due to a diagnosis of cognitive impairment, 29% (n=6) due to diagnosis of due to diagnosis of aphasia, 5% (n=1) due to diagnosis of deafness, and 28% (n=6) for a repeat visit. A total of forty two (42) patients consented to participate in the study. The majority of patients were 66 years and older (67%), with approximately 45% having some college, but no degree. Additional patient demographics are presented in Table 1. Of the 42 subjects that participated, 25 patients (60%) were identified as having adequate health literacy. Patients of adequate health literacy (SAHL-E score >14) had a mean clinic visit time of 15 minutes compared to 21.5 minutes for patients of low health literacy. The difference in total mean visit time (6.5 minutes) between health literacy groups was not statistically significant (p=0.89). Overall, the longest clinic visit was 49.5 minutes, with the shortest clinic visit time was five minutes. Results also showed that areas most focused on during the clinic visit included the comprehensive medication review and patient education (Table 2). Patients of adequate health literacy required approximately 4±4.5 minutes for disease state education, compared to 7±8.5 minutes for the low health literacy group (p=0.330).
Of the 42 patients that completed the SAHL-E assessment, 69% (n= 29) were asked to associate all 18 words, with only 9 patients with all 18 associations correct. Overall, patients were asked between 6 and 18 associations before stopping the SAHL-E and/or reaching the end of the assessment.
Discussion:
By determining the ideal visit length for patients of varying health literacy levels, a pharmacist can schedule appointments that would provide adequate time to address all issues and concerns with the patient, and to confirm understanding. There are currently no formal studies regarding the relationship of patient health literacy level and its effect on a pharmacists’ workload and/or required patient visit times. This small pilot study did not demonstrate a statistically significant difference in workload when conducting pharmacist-run clinical visits to patients of varying health literacy levels. However, a 6.5-minute difference in total clinic time between the health literacy groups suggests that more time may be necessary when scheduling patients of low health literacy. The potential differences observed in total clinic visit time may be a result of multiple factors, including patient age, education level, disease complexity, and/or accessibility to medical resources. A larger, follow-up study is necessary at this time to determine if a significant difference would be observed between new ACC visits, follow-up ACC visits, new CDM visits, and follow-up CDM visits.
Assessing health literacy at initial visits may allow clinical pharmacists to determine how a clinic visit should be conducted. A patient’s health literacy level may help determine if a patient requires extra education on their medications and disease states, or if additional time should be spent with the patient reviewing their medications and identifying drug-related problems.
Limitations:
Several limitations of this study have been identified regarding both the study population and the methods. One limitation was the study’s small sample size, which may have limited the ability to detect a difference in visit length based on health literacy. It can be theorized that a larger, multi-site study in the future may better support health literacy testing to determine appropriate clinic visit times. It would be ideal to modify the study methods to include multi sites in varying locations to better represent the patient populations served in various ambulatory care settings.
Additionally, it is common for pharmacists’ workload to continue to the next day for certain patients (i.e. consulting with another provider, follow-up with patient). However, workload that continued to other calendar days was not calculated in this study.
In regards to the methods, the observed subject (clinical pharmacist or pharmacy student) may have conducted the visit differently than they usually do because they were aware they were being observed (Hawthorne Effect). This influence may have resulted in either increased or decreased total visit time. Additionally, the total visit time may have been affected if a student pharmacist conducted the visit. A visit may have been shorter or may have lasted longer compared to one conducted by an experienced pharmacist. Furthermore, data were not collected as to what type of visit was being conducted (e.g., new ACC, follow-up CDM). A follow-up ACC visit is much different than a follow-up CDM visit, impacting the length of the visit and making comparison visits difficult.
Conclusion:
The results of this pilot study suggest additional clinic time may be necessary during visits with individuals of low health literacy, compared to adequate health literacy. Patients of low health literacy may also require additional time focused on patient education. At this time, a larger, multi-site study can determine the impact of a patient’s health literacy on a larger scale. Such results may assist in determining how appointments are scheduled to make sure patients receive the best quality of care in the allotted time frame. Additionally, it can be determined if a pharmacist should spend more time on specific discussions such as medication adherence or reconciliation in order to make sure the patient best understands and processes the medication-related information they are discussing.
Clinical pharmacists in an ambulatory care setting serving a minority population with limited resources spent more time conducting clinic visits with patients of low health literacy compared to patients with adequate health literacy. Although the findings were not statistically significant, the total visit time and time spent on certain tasks may impact a clinic’s schedule requiring extra time be allotted for patients of low health literacy, and therefore suggesting clinical significance.
References
- Glassman P. Health literacy. National Network of Libraries of Medicine. http://www.Nnlm.gov/outreach/consumer/hlthlit.html#A1. Accessed August 12, 2014.
- Nielsen-Bohlman L, Panzer AM, Kindig DA. Health literacy: a prescription to end confusion. Washington, DC: The National Academies Press; 2004.
- Johnson JL, Moser L, Garwood CL. Health literacy: a primer for pharmacists. Am J Health-Syst Pharm. 2013;70:949-955.
- Communicating with patients who have limited literacy skills. Report of the National Work Group on Literacy and Health. J Fam Pract. 1998;46(2):168-176.
- AHRQ Pharmacy Health Literacy Venter. Agency for Healthcare Research and Quality. http://www.ahrq.gov/professionals/quality-patient-safety/pharmhealthlit/index.html. Accessed August 13, 2014.
- Osterberg L, Blaschke T. Adherence to medication. N Engl J Med. 2005;353:487-497.
- Henricksen E, Kim K. Evaluation of pharmacy health literacy assessment in outpatient pharmacies. Abstract presented at: American College of Clinical Pharmacy Annual Meeting; October 13, 2014; Austin, TX.
- HealthyPeople.gov. Healthy People 2020: health communication and health information technology objectives. https://www.healthypeople.gov/2020/topics-objectives/topic/health-communication-and-health-information-technology/objectives. Accessed November 10, 2016.
- AHRQ Health Literacy Tools for Use in Pharmacies. Agency for Healthcare Research and Quality. http://www.ahrq.gov/professionals/quality-patient-safety/pharmhealthlit/tools.html. Accessed October 15, 2016.
- Meade M, Borchert J, Griffin B, Kliethermes MA, et al. Impact of health disparities on staff workload in pharmacist-managed anticoagulation clinics. Am J Health-Syst Pharm. 2011;68:1430-1435.
- Lee SD, Stucky BD, Lee JY, Rozier RG, et al. Short assessment of health literacy – Spanish and English: A comparable test of health literacy for Spanish and English speakers. HSR: Health Services Research. 2010;45(4):1105-1120.
- Harris PA, Taylor R, Thielke R, Payne J, et al. Conde, Research electronic data capture (REDCap) – a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform.2009;42(2):377-381.
ICHPeople
 Congratulations to Colleen Bohnenkamp and her husband, Nick, who welcomed their son, Theodore 'Theo' James Bohnenkamp, in to the world on October 20 at 3:44 PM. 6 lbs. 9 oz. and 20.5 inches long.
Congratulations to Colleen Bohnenkamp and her husband, Nick, who welcomed their son, Theodore 'Theo' James Bohnenkamp, in to the world on October 20 at 3:44 PM. 6 lbs. 9 oz. and 20.5 inches long.
College Connections
Rosalind Franklin University College of Pharmacy
The New President on the Block
by Jorie Kreitman, P3, Student Chapter President
I always wondered what my mark at Rosalind Franklin University of Medicine and Science (RFU) would be when I stepped foot through the doors in August of 2014. In March 2016, my time came! My name is Jorie Kreitman, and I am a third year student and the new president of the RFU chapter of ICHP. I am honored to submit this write up to KeePosted and tell you a little bit about myself, my goals as president, and how my executive board is making our organization the best organization on campus.
I have been a member of ICHP since I was in my first professional year. I wanted to be involved but didn’t know quite where I fit in. I attended all the ICHP meetings, but that’s all I did. I sat, I listened, and I watched as former executive board members spoke with passion about this organization. I knew I wanted to become more involved with ICHP but did know at what level.
My moment of clarity actually came about after experiencing a personal loss, as I have overcome a lot since my first year at RFU. My stepfather of 20 years had committed suicide. This was my defining moment as it was when I knew that hospital pharmacy practice, including pursuing a residency and eventually specializing in mental health, was where my passion lied. This was not only a moment of sadness and tragedy for me, but it was the moment I knew I had definitely chosen the right career path at the young age of seven.
Being president is a big honor and I do not take it lightly. I want ICHP student chapter at RFU to be involved with more community outreach, more fundraising, and definitely more involvement with the on-campus community. I have put into place so many goals for myself, both professionally as well as personally. I have set standards high not only because it will help me, but because it will help this organization.
My executive board is the backbone of the student chapter of ICHP at RFU and they’re the reason this organization is thriving and our goals are being achieved. We have already planned our first fundraiser. We have a photographer coming in to take professional headshots for all College of Pharmacy students, staff and faculty for LinkedIn pictures or any other professional need. The philanthropy chair has been in touch with the Midwestern ICHP student chapter and we will be participating in a joint event. This event is called “Out of the Darkness” and it raises awareness about suicide, which is something very close to my heart.
As far as our involvement on campus, we have been very successful. We had our largest group of students and faculty attend the annual meeting in Oakbrook, with 25 students and 7 faculty in attendance. Witnessing how much work my executive board has put into this organization was a moment of pure joy for me, and it reconfirmed the notion that I could not do this whole “president” thing if it weren’t for the executive board.
Looking at ICHP’s future at RFU, I see nothing but great strides forward and many future accomplishments. Within the first two months of school, our chapter of ICHP has really gone above and beyond. We plan to continue to work just as hard as we have over the summer and these first two months at school to ensure the winter and spring quarter are just as productive throughout the 2016-2017 academic year.
Midwestern University Chicago College of Pharmacy
Recognizing One of Our Own
by Paige Vortman, P-3, ICHP Historian Committee
 As student pharmacists we play a vital role in healing others. I am currently in my third year at Midwestern University Chicago College of Pharmacy and am I fortunate to take part in ICHP and gain lifelong experiences through several community service activities. It is incredible to see ICHP and other organizations at Midwestern give so much back to our community through considerable student involvement. I had the pleasure of interviewing second-year pharmacy student and our ICHP membership chair, Jenny Lin, on recently receiving the Chicago Schweitzer Fellowship Award for her outstanding community service efforts.
As student pharmacists we play a vital role in healing others. I am currently in my third year at Midwestern University Chicago College of Pharmacy and am I fortunate to take part in ICHP and gain lifelong experiences through several community service activities. It is incredible to see ICHP and other organizations at Midwestern give so much back to our community through considerable student involvement. I had the pleasure of interviewing second-year pharmacy student and our ICHP membership chair, Jenny Lin, on recently receiving the Chicago Schweitzer Fellowship Award for her outstanding community service efforts.
The Schweitzer Fellowship focuses on community service for future healthcare professionals. The fellowship accepts 30 graduate healthcare students from the Chicagoland area, including two pharmacy students. The accepted students are required to partner with an organization, design a community project, and execute the project with at least 150 direct service hours.
Jenny is partnered with Midwest Asian Healthcare Association (MAHA). When asked about her project, Jenny responded, “I will be educating patients with diabetes and hypertension on the importance of lifestyle modifications. I have pamphlets that cater to the Chinese cuisine and diet that will help [patients] better understand what types of food they can eat.” Additionally, she will host exercise classes for up to ten participants followed by brief educational sessions on dietary needs. According to Jenny, “These classes are meant to be more intimate for relationship building and will involve incentives such as portion plates and gift cards to grocery stores.”
I asked Jenny how she became involved in community service, to which she replied that she has been on mission trips to Taiwan and Honduras to teach English. She has also gone to Over-The-Rhine, Ohio several times to work with inner-city children and teenagers and Clarkston, Georgia to work with refugees. She stated, “Each of these places have been so different in terms of patient population, yet so similar in the types of needs that people have.” Jenny said she became involved in community service because she feels that she learns much more than she can give. “The population I’ve worked with has opened my eyes to disparities and barriers that exist within our society, and I have learned a lot about being patient, flexible, empathetic, and humble.”
As a first-year student, Jenny became involved with both the APhA-MTM clinics and MAHA clinics where she learned more about how to serve others as a student pharmacist. According to Jenny, “It was intimidating at first, because I felt so unconfident with my knowledge, but I’ve definitely learned a lot through those clinics. There is always something to learn not only from doing community service but also interacting with people who come from very different backgrounds or with different cultural beliefs.”
Jenny’s favorite part of participating in community service is having the opportunity to laugh with the patients. She described, “Recently, an elderly woman came to see me at MAHA. She spoke a different dialect than I did but we were still able to communicate. She asked for a portion plate and I only had one so I couldn’t give it to her so I drew it out. My drawing was terrible and could have probably been mistaken for a seven-year-old’s drawing. She saw my picture, and she laughed. She then grabbed my hand and very affectionately thanked me for drawing a portion plate out for her.” For Jenny, it’s moments like this that she loves. “[The patient] was so thankful for a picture (not even the nicest one!) of a portion plate.”
Jenny plans to continue her commitment to community service in her future career. She stated, “I think it will be awesome for pharmacists to play a huge role in fighting to end health disparities. There is a need, and if we are equipped, then we should go for it!” Jenny said the Schweitzer Fellowship opens a myriad of doors and opportunities for her to equip herself as a better pharmacist and person. “We learn a great deal about social injustice, health disparities, different types of people groups, and methods of reaching out to these groups.” Furthermore, the network allows her to meet with other future health care professionals who are also passionate about community service. “It’s a pretty great support system that this fellowship has built for us, and I hope to continue utilizing it throughout my career.”
Roosevelt University College of Pharmacy
Roosevelt University Fall Update
by Rameez Hasan, P-2, Membership Chair, Brandon Swinford, P-2, Historian/Webmaster, Samana Walji, P-2, Social Services Chair
In late October, SSHP will be hosting its quarterly journal club event. Our journal club discussions are one of the recurring events our chapter holds that has consistent participation. SSHP posts the article for the journal club in advance so students have adequate time to prepare. Together, the SSHP executive board chooses an article that the students read and prepare a journal club on. We provide templates, example completed journal clubs, and rubrics to encourage participation.
This quarter, our journal club discussion is on the article “Pioglitazone after Ischemic Stroke or Transient Ischemic Attack” from The New England Journal of Medicine. The journal club events hosted by SSHP provide students with the opportunity to improve their critical thinking skills and increase their knowledge. Fourth and second year pharmacy students must participate in the journal club if they choose to attend, while first year students can participate or attend for their edification. For first year pharmacy students, it provides them with the opportunity to attend or participate in a journal club discussion in a stress free, learning environment. They can observe their senior students, who have more experience with journal clubs, present and learn early on what a journal club is all about. The early exposure can better prepare them before they take their first drug literature class. Furthermore, it gives senior pharmacy students the opportunity to improve their journal club skills and present in front of their peers and clinical faculty member(s).
As the winter months approach, so does ASHP Midyear. For those of us still in our early years of pharmacy school, we are preparing for Midyear by creating and designing a poster to present on the behalf of the Roosevelt University College of Pharmacy SSHP. We decided to create a survey and present it to the P1 and P2 students to see how exposure to journal club discussions hosted by SSHP affect their general knowledge of biostatistics. This opportunity also provides the opportunity for students to see how journal clubs are presented to their peers. For the P1s, the journal clubs we host provide a chance for the incoming class to dip their feet into something that will become a crucial part of their curriculum and clinical skill set. For the P2s, we hope to refresh their skills of literature interpretation by providing them a chance to practice presenting a journal club to members of our clinical faculty. Whether it is reading a journal article as source for a patient case, or providing evidence for treatment procedures in a disease state, understanding journal articles is a key factor to success in pharmacy school.
More
Welcome New Members!

| New Member |
Recruiter |
| Uzma Arif |
|
| Gerald Cavanagh |
Katarzyna Pils |
| Yu-Han Chen |
Lauren Stambolic |
| Sarah Chismark |
Lauren Stambolic |
| Alicia Cobbold |
Lauren Stambolic |
| Shelby Dial |
|
| John Dicristofano |
Lauren Stambolic |
| Victoria Gavaghan |
|
| Joseph Griffin |
|
| Amanda Hjaige |
Katarzyna Pils |
| Hayley Hodgson |
|
| Tiffany King |
Laura Geswein |
| Alessandra Lagos |
|
| Daniel Majerczyk |
|
| Kaitlin Miles |
|
| Jeffrey Neal |
Lauren Stambolic |
| Jamie Nguyen |
Hina Patel |
| Taylor Page |
|
| Lauren Pare |
|
| Lauren San Juan |
|
| Darius Savickas |
|
| Zaherra Shabbir |
Lauren Stambolic |
| Tenae Shaffer |
|
| Chuxian Tang |
Lauren Stambolic |
| Alina Varabyeva |
Lauren Stambolic |
| Diana Wu |
|
| Deniz Yavas |
|
Officers and Board of Directors
2016 ELECTION RESULTS
President-elect
Travis Hunerdosse
Treasurer-elect
Kathryn Schultz
Secretary
Jennifer Arnoldi
Director-elect, Government Affairs
Chris Crank
Director-elect, Organizational Affairs
Mary Lee
Director-elect, Professional Affairs
Karin Terry
Chairman-elect, New Practitioners Network
Bernice Man
Director-elect, Northern Region
Elise Wozniak
Director-elect, Central Region
Amy Boblitt
Director-elect, Southern Region
Lynn Fromm
Special thanks to the following dedicated ICHP members who also ran for office in the 2016 Election:
Sheila Allen
Megan Hartranft
Kushal Shah
MIKE WEAVER
Treasurer 815-599-6113 mweaver@fhn.org
LARA ELLINGER Director, Educational Affairs laelling@nm.org
CARRIE VOGLER
Director, Marketing Affairs
217-545-5394
KRISTI STICE
Director, Professional Affairs
CAROL HEUNISCH Director, Organizational Affairs 847-933-6811
KATHRYN SCHULTZ
Director, Government Affairs
312-926-6961
TARA VICKERY GORDEN
Chairman, House of Delegates
618-643-2361 x2330
DAVID TJHIO
Chairman, Committee on Technology
816-885-4649
david.tjhio@cerner.com
COLLEEN BOHNENKAMP
Chairman, New Practitioners Network
BRYAN MCCARTHY
Co-Chairman, Ambulatory Care Network
VIRGINIA NASH
Co-Chairman, Ambulatory Care Network
CLARA GARY
Technician Representative
JACOB GETTIG
Editor & Chairman, KeePosted Committee
630-515-7324 fax: 630-515-6958
jgetti@midwestern.edu
Regional Directors
NOELLE CHAPMAN
Regional Director North
312-926-2547
nchapman@nmh.org
LYNN FROMM
Regional Director South
618-391-5539
Student Chapter Presidents
FLORENCE PATINO
President, Student Chapter
Chicago State University C.O.P.
SHAZIYA BARKAT
President, Student Chapter
KASIA PLIS
President, Student Chapter
Roosevelt University C.O.P.
MALLORY BELCHER President, Student Chapter Southern Illinois University Edwardsville S.O.Pmabelch@siue.edu
LEVI PILONES President, Chicago Student ChapterUniversity of IL C.O.P. lpilon2@uic.edu
TREVOR LUMAN President, Rockford Student Chapter University of IL C.O.P. tluman2@uic.edu
ICHP Affiliates
ANTOINE JENKINS
President, Northern IL Society (NISHP)
JARED SHELEY
President, Metro East Society (MESHP)
ICHP Pharmacy Action Fund (PAC) Contributors
Names below reflect donations between November 1, 2015 and November 1, 2016. Giving categories reflect each person's cumulative donations since inception.
ADVOCACY ALLIANCE - $2500-$10000Kevin Colgan
Edward Donnelly
James Owen Consulting, Inc.
Frank Kokaisl
Scott Meyers
Michael Novario
Michael Weaver
Thomas Westerkamp
LINCOLN LEAGUE - $1000-$2499
Scott Bergman
Andrew Donnelly
Ginger Ertel
Ann Jankiewicz
Jan Keresztes
Kathy Komperda
William McEvoy
Christina Quillian
Michael Rajski
Carrie Sincak
Avery Spunt
Patricia Wegner
CAPITOL CLUB - $500-$999
Margaret Allen
Sheila Allen
Rauf Dalal
Drury Lane Theatre
Kenneth Foerster
Travis Hunerdosse
Leonard Kosiba
Mary Lee
Janette Mark
Jennifer Phillips
Edward Rainville
Kathryn Schultz
Heidi Sunday
Jill Warszalek
Alan Weinstein
GENERAL ASSEMBLY GUILD - $250-$499
Tom Allen
Jennifer Arnoldi
Peggy Bickham
Jaime Borkowski
Donna Clay
Scott Drabant
Sandra Durley
Nancy Fjortoft
Michael Fotis
Jo Ann Haley
Joan Hardman
Kim Janicek
Zahra Khudeira
Ann Kuchta
Ronald Miller
Peggy Reed
Tara Vickery Gorden
Carrie Vogler
Marie Williams
SPRINGFIELD SOCIETY - $100-$249
Rebecca Castner
Noelle Chapman
Lara Ellinger
Jennifer Ellison
Nora Flint
Carol Heunisch
Lois Honan
Charlene Hope
Robert Hoy
Kati Kwasiborski
Bella Maningat
Milena McLaughlin
Megan Metzke
Katherine Miller
Kenneth Miller
Danielle Rahman
Jerry Storm
Amanda Wolff
GRASSROOTS GANG - $50-$99
Katrina Althaus
Antoinette Cintron
Jeanne Durley
Linda Grider
Heather Harper
Megan Hartranft
Erika Hellenbart
Ina Henderson
Christina Jacob
Leslie Junkins
Connie Larson
Barbara Limburg-Mancini
Brian Matthews
John McBride
Bill Middleton
Mark Moffett
Kit Moy
Gary Peksa
Daphne Smith-Marsh
Jennifer Splawski
Nadia Tancredi
Thomas Yu
CONTRIBUTOR - $1-$49
Marc Abel
Tamkeen Abreu
Trisha Blassage
Colleen Bohnenkamp
Erick Borkowski
Jeremy Capulong
Josh DeMott
Jannina Dionnio
Angelia Dreher
Tim Dunphy
Veronica Flores
Frank Hughes
Lori Huske
Vera Kalin
Levi Karell Pilones
Josie Klink
David Martin
Claudia Muldoon
Jose Ortiz
Lupe Paulino
Amanda Penland
Zach Rosenfeldt
Kevin Rynn
Cheryl Scantlen
Joellyn Schefke
Amanda Seddon
Kushal Shah
Sarah Sheley
Beth Shields
David Silva
Helen Sweiss
Steve Tancredi
Kathryn Wdowiarz
Marcella Wheatley
Tom Wheeler
Junyu (Matt) Zhang
Upcoming Events
Monday, November 14, 2016
UIC College of Pharmacy | Chicago, IL
Tuesday, November 15, 2016
Networking and dinner
Francesca's on Taylor | Chicago, IL
Thursday, November 17, 2016
Part 1: Blood Disorders: Diagnosing and Treating (non-CPE)
Mary Moody, BS Pharm
Part 2: IV Fluid Selection in Sepsis (CPE)
Craig Cooper, BS, PharmD, BCPS, BCCCP
NISHP LIVE Program
Wildfire | Oakbrook, IL
Part 2 accredited for pharmacists and pharmacy technicians | 0.75 contact hour (0.075 CEU)
Monday, December 5, 2016
Networking reception with food and cash bar
Mandalay Bay | Las Vegas, NV
Saturday, December 10, 2016
Certificate Training Program hosted by IPhA
IPhA Offices | Springfield, IL
Tuesday, December 13, 2016
Save the date! Watch the calendar and CPE News Briefs for more info.
Tuesday, January 10, 2017

Print Entire Issue