Print Entire Issue

KeePosted Info
Features
BE BOLD!
Meet John du Pré
Columns
President's Message
Directly Speaking
New Practitioners Network
ICHPeople
2014 Best Practice Award Winner: Home-Study CPE
Leadership Profile
The GAS From Springfield
College Connections
Mental Health Awareness
American Pharmacists Month at Rosalind Franklin University
Life on an Indian Reservation: APPE Edition
More
Officers and Board of Directors
Welcome New Members!
ICHP Pharmacy Action Fund (PAC) Contributors
Upcoming Events
KeePosted Info
 Illinois Council of Health-System Pharmacists
Illinois Council of Health-System Pharmacists
4055 North Perryville Road
Loves Park, IL 61111-8653
Phone: (815) 227-9292
Fax: (815) 227-9294
www.ichpnet.org
KeePosted
Official Newsjournal of the Illinois Council of Health-System Pharmacists
EDITOR
Jacob Gettig
ASSISTANT EDITOR
Jennifer Phillips
MANAGING EDITOR
Scott Meyers
ASSISTANT MANAGING EDITOR
Trish Wegner
DESIGN EDITOR
Amanda Wolff
ICHP Staff
EXECUTIVE VICE PRESIDENT
Scott Meyers
VICE PRESIDENT - PROFESSIONAL SERVICES
Trish Wegner
DIRECTOR OF OPERATIONS
Maggie Allen
INFORMATION SPECIALIST
Heidi Sunday
CUSTOMER SERVICE AND
PHARMACY TECH TOPICS™ SPECIALIST
Jo Ann Haley
ACCOUNTANT
Jan Mark
COMMUNICATIONS MANAGER
Amanda Wolff
LEGISLATIVE CONSULTANT
Jim Owen
ICHP Mission Statement
Advancing Excellence in the Practice of Pharmacy
ICHP Vision Statement
ICHP dedicates itself to achieving a vision of pharmacy practice where:
- Pharmacists are universally recognized as health care professionals and essential providers of health care services.
- Patients are aware of the training, skills, and abilities of a pharmacist and the fundamental role that pharmacists play in optimizing medication therapy.
- Formally educated, appropriately trained, and PTCB certified pharmacy technicians manage the medication distribution process with appropriate pharmacist oversight.
- Pharmacists improve patient care and medication safety through the development of effective public policies by interacting and collaborating with patients, other health care professionals and their respective professional societies, government agencies, employers and other concerned parties.
- Evidence-based practices are used to achieve safe and effective medication therapies.
- There are an adequate number of qualified pharmacy leaders within the pharmacy profession.
- Pharmacists take primary responsibility for educating pharmacy technicians, pharmacy students, pharmacist peers, other health professionals, and patients about appropriate medication use.
KeePosted Vision
As an integral publication of the Illinois Council of Health-System Pharmacists, the KeePosted newsjournal will reflect its mission and goals. In conjunction with those goals, KeePosted will provide timely information that meets the changing professional and personal needs of Illinois pharmacists and technicians, and maintain high publication standards.
KeePosted is an official publication of, and is copyrighted by, the Illinois Council of Health-System Pharmacists (ICHP). KeePosted is published 10 times a year. ICHP members received KeePosted as a member benefit. All articles published herein represent the opinions of the authors and do not reflect the policy of the ICHP or the authors’ institutions unless specified. Advertising inquiries can be directed to ICHP office at the address listed above. Image disclaimer: The image used in the Pharmacy Tech Topics advertisement is the property of © 2014 Thinkstock, a division of Getty Images.
Copyright © 2014, Illinois Council of Health-System Pharmacists. All rights reserved.
Features
BE BOLD!
2014 Annual Meeting Summary
by Trish Wegner, BS Pharm, PharmD, FASHP
The American Society of Health-System Pharmacists (ASHP) Pharmacy Practice Model Initiative (PPMI) was introduced in 2011. “The goal of this initiative is to significantly advance the health and well-being of patients by supporting futuristic practice models that support the most effective use of pharmacists as direct patient care providers." I would define this as a bold initiative or a BHAG (Big Hairy Audacious Goal); but one that can definitely be achieved. The PPMI recommendations were broken into five domains: 1) overarching principles for pharmacy practice model change, 2) specific services, 3) technology, 4) technicians, and 5) implementing change and responding to challenges.

 The 2014 ICHP Annual Meeting, whose theme was “Charting a Bold Course for Illinois Pharmacy!”, aimed to lead Illinois practitioners in this BHAG adventure by incorporating many topics related to achieving the PPMI. Imagine the keynote speaker standing on stage in a floor length bright red overcoat – now that’s bold! Even bolder was the message that Dr. Rita Shane conveyed. Dr. Shane was instrumental in the PPMI Summit where she discussed the essential elements of pharmacy practice for ensuring optimal medication use: leadership, responsibility and accountability for the medication use process, and the infrastructure of the pharmacy enterprise. In her keynote address, Dr. Shane talked about “trendbending” – the process of shaping strategy or products based upon current trends. We are in a time of health-system transformation, going from a traditional acute care focus to a health and wellness focus. Healthcare trends include: evolving reimbursement models; team-based care; nursing profession advancement; transitions of care; chronic disease management; specialty pharmacy; health literacy and adherence; and cancer care. Here is a list of Dr. Shane’s “Bold Imperatives”:
The 2014 ICHP Annual Meeting, whose theme was “Charting a Bold Course for Illinois Pharmacy!”, aimed to lead Illinois practitioners in this BHAG adventure by incorporating many topics related to achieving the PPMI. Imagine the keynote speaker standing on stage in a floor length bright red overcoat – now that’s bold! Even bolder was the message that Dr. Rita Shane conveyed. Dr. Shane was instrumental in the PPMI Summit where she discussed the essential elements of pharmacy practice for ensuring optimal medication use: leadership, responsibility and accountability for the medication use process, and the infrastructure of the pharmacy enterprise. In her keynote address, Dr. Shane talked about “trendbending” – the process of shaping strategy or products based upon current trends. We are in a time of health-system transformation, going from a traditional acute care focus to a health and wellness focus. Healthcare trends include: evolving reimbursement models; team-based care; nursing profession advancement; transitions of care; chronic disease management; specialty pharmacy; health literacy and adherence; and cancer care. Here is a list of Dr. Shane’s “Bold Imperatives”:- Keep patients at the center of our priorities and actions.
- Ensure the accuracy and safety of the patient’s medication list in the context of the whole patient and in collaboration with the healthcare team.
- Recognize that ensuring safe use of medications is not limited to the brief time that patients spend within our walls.
- Measure what we do in terms that are relevant to decision-makers at the health-system, health professional and health policy levels.
- Remember that progress is the outcome of each interaction that we have.
- Each encounter presents us with an opportunity to and a responsibility for demonstrating our value to each stakeholder, especially to our patients.
- An indicator of progress in transforming pharmacy will be public demand. – Bill Zellmer
- Progress will be achieved when our patients ask, “Where is my pharmacist?” – Rita Shane
So how can you be a trendbender at your institution? Are you incorporating the goals of the PPMI? Handouts for the presentations at the Annual Meeting are still available on the ICHP website if you were not able to attend, but still would like to see what our keynote and others shared with the attendees.
Through the Technology and Management sessions we discussed how to incorporate technology to improve patient safety and how to train both pharmacists and technicians in the area of informatics, a growing specialty in pharmacy practice. This addressed the PPMI recommendation of “Sufficient pharmacy resources must be available to safely develop, implement, and maintain technology-related medication-use safety standards.”
The pharmacy technician session showcased the unique roles that pharmacy technicians are assuming, thereby freeing pharmacists to perform more clinical functions and ultimately improve patient care and satisfaction – one of the key areas of the PPMI summit agreement. A major function of pharmacy technicians is the preparation of sterile compounds, prompting a presentation on processes and procedures for maintaining a clean environment for compounding. In addition, there was a very interactive and entertaining session on how to communicate effectively with each other in the workplace setting. It was so well received that we are repeating it at the Spring Meeting.
Implementing new pharmacy practice models can be achieved through the structured integration of pharmacy students and residents. As such, the Planning Committee incorporated sessions on how to establish or expand pharmacy residency programs in Illinois. In order to achieve the goal, of all new graduates of pharmacy schools being residency trained by 2020 if they have direct patient care, we must expand the number of residency positions available. ICHP continues to foster the development of residency programs and has incorporated this goal in its strategic plan.
Addressing the goal of pharmacists being responsible and accountable for patients’ medication-related outcomes, the Annual Meeting included presentations on ambulatory care services such as a Hepatitis Clinic; updates and review of new national disease state guidelines; review of recent literature; overview of new therapies; and interpretation of the primary literature.
So have we achieved the BHAG? Not yet, but we are well on our way. With continued innovative practice and strategic planning, pharmacy will accomplish all that has been set by the PPMI. ICHP will continue to offer education in key areas related to this audacious goal.
If you are still not aware of the PPMI, please go to http://www.ashpmedia.org/ppmi/ and learn more. Even better, complete the scorecard for your institution to see how you compare to other hospitals. This is a great project for a new practitioner, resident or student.
The meeting drew a record 561 in attendance including numerous students and residents, which is an almost 7% increase over last year’s meeting and Gala celebration. Seeing lots of new and young faces was exciting. We want to thank all the students and residents who took part in the Annual Meeting and hope you had an opportunity to network during the Residency Showcase and NPN Mixer. The Residency Roundtables has become so popular that we are going to have to find alternative ways to meet the needs of all the students. That’s a good problem to have. We’ll be looking at the student evaluations to get some ideas.
With decreasing educational grants being awarded for programming, support from our industry partners during the Exhibit Program is key to maintaining lower registration costs for you. We greatly thank the 56 vendors who participated in the Exhibit Program! Special thanks also to the following meeting sponsors:
- Cubist – Platinum Sponsor
- Novo Nordisk – Platinum Sponsor
- Baxter – Gold Sponsor
- Daiichi Sankyo – Gold Sponsor
- Abbvie – Silver Sponsor
- Amgen – Silver Sponsor
- Celgene – Silver Sponsor
- CSL Behring – Sliver Sponsor
- Kit Check, Inc. – Silver Sponsor
- McKesson Pharmaceuticals – Silver Sponsor
We do not plan any educational programming during the Exhibit Program to encourage all our attendees to visit with our vendors so that they continue to partner with us and exhibit. Without their support, ICHP would have to increase the price of the meeting registration fee to cover expenses. So next year, please use the time to network with our industry partners and learning about new products and services they offer.
Stars were shining brightly during the Award Ceremony. The Shining Star award was created to recognize volunteer members who have stepped up their volunteer involvement a notch over the past year. The 2014 Shining Stars are:
- Fatima Ali
- Pete Antonopoulos
- Jennifer Arnoldi
- Brian Hoff
- Abby Kahaleh
- Oksana Kucher
- Bernice Man
- Janene Marshall
- Ed Rainville
- Colleen Simmons
 The Amy Lodolce Mentorship Award was created in memory of Amy Lodolce who passed away in August of 2012. Amy was a great mentor to her students, residents, and colleagues. Nominees for this award must meet the following criteria: 1) be a current ICHP pharmacist or pharmacy technician member; 2) be a preceptor, professor or mentor of students, residents, technicians and/or new practitioners; 3) demonstrate efforts to advance the practice of pharmacy; 4) demonstrate strong mentorship capabilities; 5) exhibit clear community service participation; and 6) have impacted the nominator’s career. Amy’s husband, James Lodolce, presented the award to Andy Donnelly of the University of Illinois Hospitals and Clinics for his long-term commitment to mentoring students, residents, young pharmacists, and technicians, and his dedication to advancing pharmacy practice worldwide. We were also honored to have Amy’s mother, Diane Vuletich, in attendance.
The Amy Lodolce Mentorship Award was created in memory of Amy Lodolce who passed away in August of 2012. Amy was a great mentor to her students, residents, and colleagues. Nominees for this award must meet the following criteria: 1) be a current ICHP pharmacist or pharmacy technician member; 2) be a preceptor, professor or mentor of students, residents, technicians and/or new practitioners; 3) demonstrate efforts to advance the practice of pharmacy; 4) demonstrate strong mentorship capabilities; 5) exhibit clear community service participation; and 6) have impacted the nominator’s career. Amy’s husband, James Lodolce, presented the award to Andy Donnelly of the University of Illinois Hospitals and Clinics for his long-term commitment to mentoring students, residents, young pharmacists, and technicians, and his dedication to advancing pharmacy practice worldwide. We were also honored to have Amy’s mother, Diane Vuletich, in attendance.
The Industry Award was presented to David Tjhio of Cerner Corporation. This award is given to a member of industry who steps up and makes unique contributions to health-system pharmacy in Illinois and supports and encourages participation by others in ICHP through membership, meeting attendance and organizational activities. David has served as the ICHP Technology Committee Chair since 2001 and has worked to support pharmacy practice and improve patient safety as part of his job as well as through the Council.
The New Practitioner Leadership Award was presented to Diana Isaacs of Chicago State University. Diana epitomizes this award through extensive involvement in ICHP through service as the NPN Chair, member of the ICHP Strategic Planning Committee, the Social Media Committee, the Division of Professional Affairs and the Annual and Spring Meeting Planning Committees. She also is the Co-Advisor for the CSU Student Chapter. Diana is a great example for all new practitioners and is very deserving of this award.
The Student Chapter Award went to the Chicago State University College of Pharmacy chapter for promoting the mission of ICHP through their many activities throughout the year. The selection criteria are divided into three categories: presence of the student chapter at ICHP activities, activities the student chapter uses to promote the mission of ICHP, and documentation of how the activities promote the ICHP mission through submission of an essay.
The Outstanding Volunteer Award was presented to Travis Hunerdosse of Northwestern Memorial Hospital for his service as the Director of the Division of Educational Affairs over the last three years; and for chairing the Annual and Spring Meeting during this same period of time. This award is presented by the Executive Committee to the volunteer leader of ICHP who has stepped-up and through outstanding effort has significantly made many accomplishments on behalf of the Council.
The President’s Award was given by President Mike Fotis, to Jennifer Ellison of OSF Saint Francis Medical Center in Peoria. The President’s Award recognizes a member of ICHP for contributions to the Council that are considered above and beyond the normal volunteer member. These contributions may be on behalf of ICHP or pharmacy in general and may be made at the local, state, or national level. The President of ICHP has the sole responsibility of the selection of the recipient. Jennifer is a Drug Information Pharmacist and PGY1 Pharmacy Residency Director and served as the Division Director of Marketing Affairs. She has served as the Central Region Director for which she received the Outstanding Volunteer Award in 2010.
ICHP’s highest award, the Pharmacist of the Year Award, was given to Mary Lynn Moody for her years of service to the profession. She is currently the Director of Business Development and Clinical Associate Professor at the University of Illinois at Chicago College of Pharmacy. Mary mentors pharmacy students in the UIC Drug Information Center and guides them on to great practices. Her entrepreneurial acumen has resulted in the creation of many new services through UIC including national DI services, contracting with the state to provide prior authorization services while incorporating pharmacists more clinically into the Medicaid program. She has served on the ICHP Board including as the President of the Council. Mary is very active politically in the state and can always be found at the Illinois Pharmacy Legislative Day.
ICHP congratulates all the award winners who truly are bright stars not only for ICHP but also for Pharmacy! ICHP also wishes to thank Mike Fotis, Immediate Past-President, for his wisdom and bold leadership over the past two years as President-Elect and President. ICHP welcomes Linda Fred to take over “the gavel” and marshal the organization to continued collaboration.
ICHP helped to build the boat, now it is up to every pharmacist, pharmacy technician and pharmacy student to raise their sails and chart a course for pharmacy – be bold!
Please join ICHP and MSHP at the Spring Meeting, March 20-21, 2015 at the St. Charles Convention Center in St. Charles, Missouri where we will be “Growing Pharmacy Together”.
Meet John du Pré
by John Lee du Pré, PharmD candidate 2015, University of Illinois - Rockford College of Pharmacy
 Hello, my name is John Lee du Pré and I am a 4th year pharmacy student at the University of Illinois at Chicago College of Pharmacy in Rockford, Illinois. I grew up in Missouri and when I graduated from high school I joined the United States Navy. After 6 years in the Navy I decided to return to school. I graduated from Lincoln Land Community College in 2002 then transferred to Northern Illinois University to study philosophy. I graduated in 2004 and started graduate school in 2005. After reexamining my goals and priorities, I decided to change directions and start the pharmacy journey.
Hello, my name is John Lee du Pré and I am a 4th year pharmacy student at the University of Illinois at Chicago College of Pharmacy in Rockford, Illinois. I grew up in Missouri and when I graduated from high school I joined the United States Navy. After 6 years in the Navy I decided to return to school. I graduated from Lincoln Land Community College in 2002 then transferred to Northern Illinois University to study philosophy. I graduated in 2004 and started graduate school in 2005. After reexamining my goals and priorities, I decided to change directions and start the pharmacy journey.
I met my wife in Italy while on assignment for the Navy in 1993. We have three children (all girls) ages 15, 13, 10 and our 20th wedding anniversary will be next April! I have many passions/hobbies but my favorite activities are spending time with my family, cooking, traveling, learning new things, and goal setting/achieving.
 I have several goals for this rotation. First, I want to understand the professional relationship between ICHP, government, and pharmacy members. Second, I hope to have many opportunities to research, organize and communicate findings regarding pharmacy law and to critically analyze the impact ICHP has on the profession of pharmacy. Finally, I hope to develop my self-directed learning skills to help advance my pharmacy education. Overall I know the ICHP rotation will give me an appreciation for association work and the positive impact ICHP has on our profession.
I have several goals for this rotation. First, I want to understand the professional relationship between ICHP, government, and pharmacy members. Second, I hope to have many opportunities to research, organize and communicate findings regarding pharmacy law and to critically analyze the impact ICHP has on the profession of pharmacy. Finally, I hope to develop my self-directed learning skills to help advance my pharmacy education. Overall I know the ICHP rotation will give me an appreciation for association work and the positive impact ICHP has on our profession.
Columns
 President's Message
President's Message
Inaugural Address: Collaboration
by Linda Fred, ICHP President
It’s a great pleasure to be standing in front of you today as the organization’s next President. First, I’d like to thank Mike Fotis again for his excellent leadership of the organization this past year. I’d also like to recognize Scott and our ICHP staff for their support.
I graduated from college – the first time – 30 years ago now. I feel like I’ve literally grown up, professionally, with ICHP. The people in this room are my professional family. The professional connections we build throughout our careers have a profound effect on the paths those careers take and my path has certainly been driven, at times, by my ICHP connections. I’ve had the opportunity this weekend to share time with so many incredible practitioners of the profession – people who have served as the trend-setters, have set the standards for exceptional practice, have been the mentors, and who have been leaders not just within ICHP, or even throughout the state, but truly at a national level. It’s a tremendous honor to just be in the presence of the past and future leadership group of this organization, and I’m thankful every day for my ICHP family, who has helped me in my career just by setting that great example of professional practice and industry leadership.
I’ve listened to a fair number of these presidential inaugural addresses over the years, and I have a habit of thinking, “What grand plans would I lay out for the year ahead?” (So, for those of you who were panicking because I didn’t write this speech until last night – what you didn’t know was that I’ve been writing it over and over in my head for probably ten years.) One thought that is a perennial inclusion in the inaugural address in my head is, “What an exciting time it is to be a pharmacist!” And it’s true again this year. We are so fortunate to be in a profession that is so demanding and challenging and yet rewarding and so full of opportunity – and the types and number of opportunities just keep expanding for both our pharmacists and our technicians. As the healthcare dollars continue to contract, there’s greater demand for every member of the healthcare team to operate at the top of their scope and interact successfully with every other member of the team.
That leads me really to the meat of my address. One of my first official duties as President was to select a theme for my term. I’ve actually been joking about that and have told several people this weekend that about all I’ve done as President so far is pick themes and go to parties…I feel like the organization’s newly elected Social Chair. But it came to me that being the Social Chair is definitely part of my responsibility, and also consistent with my chosen theme, which is collaboration.
We’ve heard quite a bit about collaboration this weekend. In our first presentation on Thursday morning, we heard about a great collaboration by an Emergency Room Pharmacist helping provide a novel medication delivery system for patients needing emergency care but with no IV access available. Dr. Rita Shane talked about team-based care and medical homes and the importance of collaboration in providing optimal care to our patients across the continuum. During the smart pump presentations on Thursday, the presenters talked about the pump selection and implementation teams and what an integral part the pharmacists played. At our House of Delegates meeting Thursday night, we had a delegate recommendation about reaching out to our professional peers in non-traditional settings. A new plank in the organization’s strategic plan is to look for common ground with other professional groups such as those representing hospitalists and nurse practitioners. Then we heard about some model collaborative practice settings from the speakers who are in the hepatitis clinics. At our Town Hall Meeting yesterday, we had a great start to what must inevitably be a much bigger conversation about ICHP’s relationship with IPhA and what that should look like in the future, and whether we can truly be “one voice” for the profession in the state of Illinois.
Collaboration is our new imperative. We have to collaborate with our patients and their in-home caregivers as the costs of readmissions threaten health system reimbursement. We have to collaborate with our social services and case management providers to address the non-medical needs that affect the medical outcomes because if patients can’t afford their medications, they will come back to the hospital and probably sicker than when we saw them the first time. We have to collaborate with our administrators to continue to demonstrate our value in current services and to identify new service lines where pharmacists are uniquely prepared to improve patient outcomes. We have to collaborate with our colleges of pharmacy because they are training our future leaders. We have to collaborate with other professional associations both within and outside pharmacy in order to achieve our professional goals – particularly recognition as providers.
And finally, we must collaborate with each other to advance our practice. One of the great strengths of this organization is our willingness to share ideas with one another. I would be remiss if I didn’t take a moment to encourage all of you to be active participants in your own – and our collective – professional development journey. I have a saying that I’m fond of, and I’m sure my employees are sick of hearing it, but you’re a new audience, so I’m going to share it with you today. Decisions are made by the people who show up. So, my charge to you today is…show up. Join a committee, or submit a poster, or go to a mixer. Do something! Take that first step toward active membership. Be part of, without a doubt, one of the best professional pharmacist associations in the country.
I’m looking forward to a great year as your President. I hope you will join me!
Thank you.
 Directly Speaking
Directly Speaking
Illinois House Heroin Task Force: Focusing On the Problems
by Scott A. Meyers, Executive Vice President
On Tuesday, October 7th, a small group of pharmacy profession representatives met with Representatives Lou Lang (D) and Dennis Reboletti (R), co-chairs of the Illinois House of Representatives Heroin Task Force in downtown Chicago to address an issue that currently plagues Illinois. Reps. Lang and Reboletti asked the pharmacy community for help with this critical and growing problem. The profession was represented by Rob Karr, President of the Illinois Retail Merchants Association (IRMA); Garth Reynolds, Executive Director of the Illinois Pharmacists Association (IPhA); Joel Baise, Walgreens; Kathryn Schultz, Gary Peksa and Scott Meyers, ICHP’s Director of Government Affairs, members of the Division of Government Affairs, and Executive Vice President, respectively. (Kathryn and Gary attended at the request of House staff and me.)
Representative Lang began the meeting with a description of the Task Force (39 members of the House from both sides of the aisle – that means it is bi-partisan) and then highlighted the goals of legislation. Important to the Task Force was creating language that could be voted on in November during the Veto-session of the Illinois General Assembly. That’s a very ambitious plan. The primary goals of the Task Force are:
- Reduce deaths from heroin overdose
- Reduce access to prescription opioids that may lead to heroin use
- Strengthen efforts to combat heroin use and addiction in Illinois
Rep. Lang discussed three major areas the bill would address:
- Over-prescribing of opioid medications
- Pharmaceutical Take Back Programs
- Strengthening the Prescription Drug Monitoring Plan (PMP)
The Representatives questioned the value of flagging patients who receive prescriptions for controlled substances from six doctors or six pharmacies in a 30-day period and the limited value of then sending the prescribers involved with that patient a letter advising them of the situation. Should or could the current PMP processes be tightened? The Task Force would like to use prescriber data from the PMP to identify those physicians who prescribe high quantities of controlled substances. Is the number of prescriptions reasonable for their area of practice? The question of auto-registration to the PMP at the time of physician licensure renewal by IDFPR (Illinois Department of Financial and Professional Regulation) was raised as a means to encourage and facilitate physician utilization of the PMP. Are physicians actively logging onto the PMP to build their accounts (currently a voluntary process) and would auto-registration facilitate use of the PMP by more doctors? They asked if pharmacy had any barriers in accessing the PMP. The answer we provided was not to our knowledge.
The Task Force does not want to encourage or allow fishing trips by the DEA or law enforcement, taking large volumes of data to identify frequent controlled substance users, but would condone the use of PMP data by IDFPR to follow-up with frequent prescribers. This will likely be a problem for the Illinois State Medical Society.
Rob Karr stated to Reps. Lang and Reboletti that he felt that since the physicians constantly maintain that they are the “gatekeepers” to the healthcare process, then isn’t it appropriate that they (the physicians) be required to check the PMP prior to prescribing controlled substances? (At least whenever the physician is dealing with a new patient.) Having the PMP interface with electronic prescribing software could facilitate this process and reduce the time burden on the doctors. That’s a discussion that needs to occur with e-prescribing software companies. It was the pharmacy representatives’ consensus that the pharmacist should not be required to check the PMP unless the physician is at least required to do the same.
We explained to Reps. Lang and Reboletti that currently the PMP is not a real-time tool but can be up to 7 days behind in showing filled prescriptions. The question was asked if making the PMP a real-time tool would improve detection of doctor and pharmacy shoppers. It was reported that Oklahoma has a real-time system that is frequently down because of the additional maintenance and load. In addition, switching to real-time is costly for both pharmacies and the State.
Pharmacy Take Back Programs were discussed at length. Rep. Lang suggested that the bill could require all pharmacies to participate in these programs in order to remove more prescription medications from homes. Those in attendance raised issues of space, security and cost requirements for these programs. The Task Force believes that these programs should be widespread and on-going. Occasional local programs are not sufficient to help solve the problem of access to opioid products by teenagers and young adults, and additionally, law enforcement agencies are not willing or able to take on these programs by themselves. The Representatives were understanding of the cost issue and also did not realize their impact on work space, work flow and overall security of the pharmacy. They were also unaware that many of the meds that are returned with these programs are not easily identifiable because they have been removed from their original containers or were originally provided to the patients in Med Paks rather than prescription bottles.
Naloxone availability to rescue overdose victims was also discussed and it was a unified recommendation by the pharmacy representatives in the room that intranasal (IN) administered naloxone should be the only medication considered safe for distribution to the general public and law enforcement. There are also concerns with providing a prescription medication to someone other than the potential patient. The state would have to provide some sort of standing order for pharmacies to be able to prescribe and dispense intranasal naloxone to a family member or concerned friend of a heroin user. Rep. Lang said that could be written into the bill. There was some limited concern by the Representatives for preventing dealers from buying the intranasal naloxone for their customers as a means to maintain business, but the risk/value didn’t seem too significant of an issue in making naloxone more accessible overall.
Representative Lang asked the pharmacy organizations to come up with some proposed language within 30 days that would help the Task Force accomplish its goals while hopefully not causing significant burden on pharmacies. Much of this will impact community pharmacy practice and hospital pharmacies alike, not necessarily just those with outpatient pharmacies. It may be quite possible that hospitals that have pharmacies within their walls would have to provide access to a Take-Back program and the inpatient pharmacy would be responsible.
The new DEA rules that allow pharmacies to now “Take Back” unused and expired controlled substances may be used by the General Assembly to force every pharmacy to do just that! ICHP’s Division of Government Affairs will be working diligently to make sure whatever the Task Force comes up with is reasonable and fair to all.
New Practitioners Network
ICHP Walks to Cure Diabetes
by Colleen Czerniak, PharmD, BCPS
 On October 5, 2014, a cool autumn morning welcomed over 7,500 people, 17 of which represented Team ICHP, to stroll along the Lakeshore path near Montrose Harbor to bring awareness to and fund research for Type 1 Diabetes (T1D) and the Juvenile Diabetes Research Fund (JDRF). Among those participants, Team ICHP, wearing bright orange shirts reading, “orange you glad hospitals have pharmacists?” celebrated its inaugural participation in the Ron Santo Walk to Cure Diabetes. The Lakefront location was one of seven JDRF walks across the Chicagoland area, which raised an astonishing $3.9 million this year!
On October 5, 2014, a cool autumn morning welcomed over 7,500 people, 17 of which represented Team ICHP, to stroll along the Lakeshore path near Montrose Harbor to bring awareness to and fund research for Type 1 Diabetes (T1D) and the Juvenile Diabetes Research Fund (JDRF). Among those participants, Team ICHP, wearing bright orange shirts reading, “orange you glad hospitals have pharmacists?” celebrated its inaugural participation in the Ron Santo Walk to Cure Diabetes. The Lakefront location was one of seven JDRF walks across the Chicagoland area, which raised an astonishing $3.9 million this year!
The day commenced with an opening ceremony sharing inspiring testimonials from actual T1D sufferers, which was then followed by the Star Spangled Banner. Surrounding the stage were tents from local vendors, such as Corner Bakery who were offering bagels and juice and handing out free giveaways. As our team members arrived, we gathered at the ICHP table where we put faces to names, met several new ICHP members and students, and caught up with those we already knew.
When we began our walk, I couldn’t help but think of the flu shot I had received the day prior and the lingering discomfort it left in my arm. That’s when reality sunk in and I looked around and thought of all the little kiddos walking beside me that were suffering from T1D. I then thought of those that I knew suffering from T1D. My cousin is a mother of five children, two of whom suffer from T1D, the youngest of which was diagnosed at only three years of age. Can you imagine the struggle, pain, and confusion of poking and injecting a toddler multiple times per day? Or attempting to count carbohydrates and calculate insulin requirements for two young children? Every. Single. Day. This is a disease that not only impacts the patient, but also greatly impacts their loved ones and family members.
Over 30,000 people are diagnosed with T1D each year. Worldwide, the JDRF is the largest nonprofit funder of T1D research, and the Walk to Cure Diabetes is its largest fundraising event with over 900,000 walkers each year. The Lakefront walk was merely one of 212 walks across the country, which raise millions of dollars each year to fund breakthrough research, such as the artificial pancreas and encapsulated beta cell therapies.
Beautiful Lake Michigan glistened in the sunlight during our walk as we shared stories, mingled with new people, and enjoyed the fresh autumn air. Upon crossing the blue archway of the finish line, we were greeted with upbeat music and choreographed dancing and a variety of sandwiches and snacks to reward us for a walk well done. After lunch, several of us participated in Project S.N.A.P.’s The Community Mosaic Mural Program, in which we created individual, small pieces of art reflecting our experiences with or hopes for T1D. Our individual art pieces will be combined, mosaic style, with artwork from walks across the country to create a giant mural which transforms our individual messages into one unified group message: Hope for a World without Type 1 Diabetes.
What equated to less than a two hour time commitment to participate in the walk, resulted in invaluable camaraderie, networking, and the satisfaction of supporting a great cause. On behalf of Team ICHP, I would like to sincerely thank every person that joined us on the walk, and every person that donated to help Team ICHP reach our fundraising goal in our first annual Walk to Cure Diabetes! We raised $1540, just above our goal of $1500! Your generosity is crucial in funding life-saving, innovative research to create a world without T1D. Lastly, I ask you to consider joining us next year as we walk to turn Type One into Type None!
ICHPeople
Congratulations to the SIUE Student Chapter on receiving the Outstanding Professional Development Project Award! They will be presenting their winning project at the Student Society Showcase at the ASHP 2014 Midyear Clinical Meeting and will be recognized during the Pharmacy Student Forum Awards Ceremony.
 The Pediatric Pharmacy Advocacy Group awarded SIUE's Dr. Lisa Lubsch its 2014 Presidential Citation for Service during its annual meeting May 2 in Nashville. Lubsch, PharmD, is a clinical associate professor in the Department of Pharmacy Practice at SIUE’s School of Pharmacy.
The Pediatric Pharmacy Advocacy Group awarded SIUE's Dr. Lisa Lubsch its 2014 Presidential Citation for Service during its annual meeting May 2 in Nashville. Lubsch, PharmD, is a clinical associate professor in the Department of Pharmacy Practice at SIUE’s School of Pharmacy.“I’m surprised, delighted and honored to be recognized in this way by a group of my true pediatric pharmacy peers,” said Lubsch. “There is nothing greater than being acknowledged by those who share the same passion for working with and helping children.”
Additionally, Dr. Lisa Lubsch has been appointed to lead the Pediatric Pharmacy Advocacy Group-University (PPAG-U) initiative. As part of her role beginning in spring 2015, Lubsch will direct section leaders from 15 areas of expertise in the field of pediatric pharmacy.
2014 Best Practice Award Winner: Home-Study CPE
Impact of Pharmacist Involvement in the Transitional Care of High-Risk Patients through Medication Reconciliation, Medication Education, and Post-Discharge Callbacks
by Arti Phatak, Pharm.D.; Brooke Ward, Pharm.D., BCPS; Rachael Prusi, Pharm.D.; Elizabeth Vetter, Pharm.D.; Michael Postelnick, BS Pharm, BCPS (AQ Infectious Diseases); and Noelle Chapman, Pharm.D., BCPS; Northwestern Memorial Hospital
LEARNING OBJECTIVES FOR PHARMACISTS AND PHARMACY TECHNICIANS:
- Review common causes for inpatient readmissions.
- Discuss areas of improvement for continuity of care.
 ACCREDITATION:
ACCREDITATION: This program is sponsored by the Illinois Council of Health-System Pharmacists. The Illinois Council of Health-System Pharmacists is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education.
This program is will provide 0.5 contact hours (0.05 CEUs) of pharmacy continuing education for pharmacists. This program is free to ICHP members only.
ACPE Universal Activity Numbers:
0121-0000-14-051-H05-P
0121-0000-14-051-H05-T
Type of Activity: Knowledge-based
NEW - Pharmacy Technicians may attend Pharmacist (P-specific) programs for credit through 2014. However PTCB is changing their continuing pharmacy education requirements in 2015. Beginning in 2015, PTCB will require CPhTs to submit 20 hours of pharmacy technician-specific (‘T-specific’) continuing pharmacy education (CPE) to qualify for recertification. Pharmacy technicians will no long be able to use Pharmacist only or P-specific CPE. In addition, PTCB will reduce the number of allowable CPE hours earned through in-service training from 10 to 5. Please advise all pharmacy technicians at your site of this pending change. As an ACPE accredited provider, ICHP will continue to include Technician specific programming in most of our CPE programming.
FACULTY DISCLOSURE: It is the policy of the Illinois Council of Health-System Pharmacists (ICHP) to ensure balance and objectivity in all its continuing pharmacy education programs. All faculty participating in any ICHP continuing pharmacy education programs are expected to disclose any real or apparent conflict(s) of interest that may have any bearing on the subject matter of the continuing pharmacy education program. Disclosure pertains to relationships with any pharmaceutical companies, biomedical device manufacturers, or other corporations whose products or services are related to the subject matter of the topic.
The intent of disclosure is not to prevent the use of faculty with a potential conflict of interest from authoring a publication but to let the readers know about the relationship prior to participation in the continuing pharmacy education activity. It is intended to identify financial interests and affiliations so that, with full disclosure of the facts, the readers may form their own judgments about the content of the learning activity.
The authors’ submission has been peer reviewed with consideration and knowledge of these potential conflicts and it has been found to be balanced and objective. The authors have no real or apparent conflict(s) of interest that may have any bearing on the subject matter of this continuing pharmacy education program.
INSTRUCTIONS FOR OBTAINING YOUR CPE CREDIT:
Instructions for joining CESally.com as an ICHP Member to ACCESS Best Practice Journal CPE
We are transitioning to a brand new continuing pharmacy education (CPE) website called CESally.com. You will be able to see the Best Practice CPE programs and access them for credit, once you sign in to CESally and select ICHP as your association. Step I below is for those who do not have a CESAlly.com account yet. If you already have a CESally.com account, please go to Step II.
Step I. Setting up your ASSOCIATION account on CESally.com:
- Your will receive an email from “ICHP (via CE Sally)” today, November 6, 2015.
- Open the email and “Please click on the link to accept this invitation.”
- Create an account – add your NABP eProfile ID and birth date as mmdd.
- Click on “Your Account”
- Select “Association Invitation” on the right hand side of webpage.
- You will see a green bar saying invitation accepted.
- Click on “Featured CE” tab at top of page.
- Type in a key word from either title in the Search box and enter.
- Select the Best Practice Award program and follow the steps to claim your CPE credit.
(Complete the Post test and evaluation.)
Step II. If you have already set up your CESally.com account, but did not set up your Association link for member free programming, go to “Your Account” page. On the right side you will see “Professional Associations”. Click on that link. Select ICHP. You should now see the private members’ only programs. Follow #9 above to complete your Best Practice CPE process.
Background
From 2007 through 2011, Medicare claims showed a 19% all-cause 30-day readmission rate.1 Previous literature has shown that up to 47% of hospital readmissions could be classified as preventable.2 As this area continues to be identified as a non-reimbursable cost-reduction target, hospitals are investigating various interventions that can reduce readmission rates. As a potentially underutilized member of the healthcare team, pharmacists can play a valuable role in preventing medication errors and adverse drug events (ADEs) while optimizing medication outcomes to improve patient care.
While there are many potential factors contributing to likelihood of readmission, one consistently identified aspect is the lack of acceptable transitional care, which refers to the safe and timely transfer of a patient between health care settings or health care practitioners.
Prior studies have consistently demonstrated the high likelihood of ADEs and patients’ lack of knowledge regarding medications post-discharge, both of which can lead to readmission. Forster and colleagues, in two separate trials, found that 19-23% of patients experienced an adverse event within five weeks of discharge from an inpatient visit; 66-72% of which were drug related and approximately one-third of which were deemed preventable.3,4 According to a study by Schnipper and colleagues, medication review, discharge counseling, and post-discharge phone calls were all associated with a significantly lower rate of preventable ADEs 30-days after hospital discharge.5 While overall pharmacist participation has shown positive patient-related outcomes, the impact of pharmacist involvement on readmission rates has not been consistently demonstrated. This study evaluated the impact of the pharmacy team on the currently fragmented transition between care settings in a unique combination by utilizing the pharmacist during medication reconciliation, discharge, and at three points post-discharge.
Methods
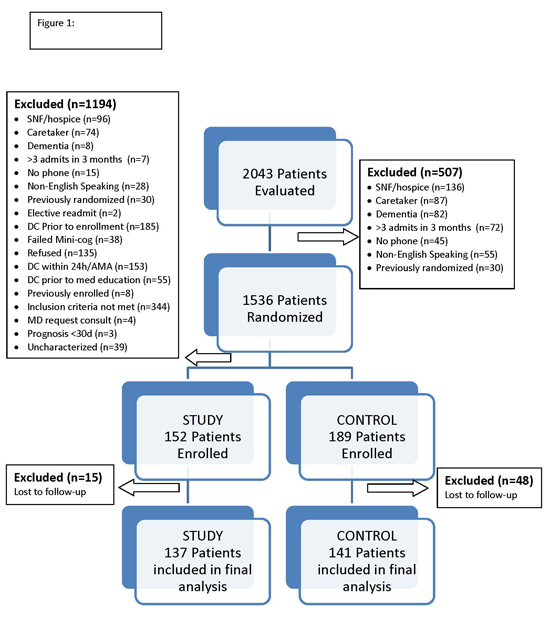
All patients admitted to one of two designated internal medicine units at Northwestern Memorial Hospital, were eligible for participation in the study. Inclusion criteria were: discharged to home, discharged on more than three prescription scheduled medications, or discharged with at least one of the following high-risk medications: anticoagulants (including antiplatelets), anti-diabetics, immunosuppressants, or anti-infectives. Exclusion criteria included: failed Mini-Cog Screening assessment tool, unable or unwilling to provide informed consent, lack of a personal phone number, non-English speaking, subsequent elective readmission within 30 days of initial visit, more than three previous hospital admissions in the past two months, discharge other than home, anticipated length of survival less than 3 months, discharged within 24 hours of admission, discharged against medical advice, or discharged before medication education was conducted (Figure 1). All patients who met inclusion criteria provided informed consent, received a Mini-Cog screening assessment, and received the REALM-R to evaluate health literacy. Patients were randomized to receive either usual care or pharmacist-directed medication evaluation and management (Figure 2). Patients included in the study were contacted by phone with three attempts on consecutive days. Patients who experienced an inpatient readmission or emergency department (ED) visit to the study center were not contacted after the point of readmission.
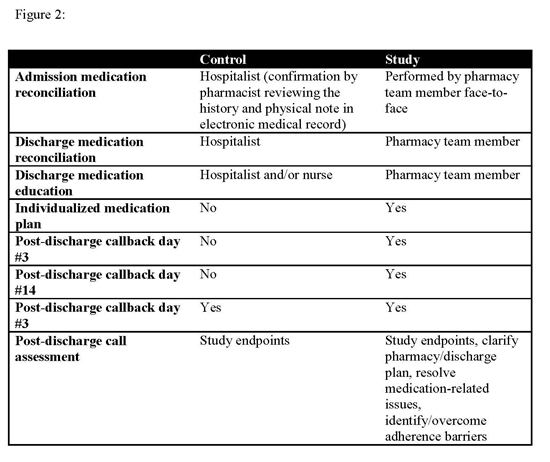
Patients enrolled in the control group received usual care, which included medication reconciliation based off the history and physical performed by the admitting physician and discharge instructions and medication counseling provided by the physician or nursing staff. Control patients received one post-discharge phone call at 30 days to assess ADE occurrence, inpatient readmissions, and ED visits.
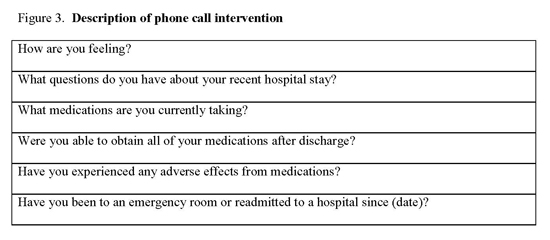
Patients enrolled in the study group received face-to-face medication reconciliation on admission by a pharmacist or a pharmacy student and a personalized medication plan developed by the pharmacist and discussed with the physician. Any medication discrepancies were addressed prior to the discharge instructions being given to the patient. Medication counseling was performed at discharge by the pharmacist or pharmacy student. Patients received three phone calls at 3, 14 and 30 days post-discharge. The calls were aimed at clarifying the pharmacy plan at discharge, resolving any unanswered questions or medication-related issues, and identifying and overcoming any barriers to adherence. If a discrepancy from the discharge plan was identified, the patient’s primary care physician or pharmacy was contacted for clarification. (Figure 3).
This study was funded through a grant provided by the American Society of Health-System Pharmacists Foundation.
Data collected from patients included demographic data (age, sex), reason for admission, number of medications at time of discharge, number of high-risk medications prescribed at time of discharge, length of stay, ADEs, inpatient readmission or ED visit, and the reason prompting readmission or ED visit. Only the first occurrence was counted for patients with both an ED visit and an inpatient readmission. HCAHPS scores for the domain of “patient knowledge of medications at time of discharge” were collected for a period of six months prior to the study period and throughout the study period. It was estimated that a sample size of 150 patients in each group would provide 80% power to demonstrate a 20% improvement in ADE rates in the study group. Data were analyzed statistically utilizing Fischer’s exact, chi-square and Student’s t-tests as appropriate.
Results
Over the course of seven months, 341 patients were enrolled in this study, 189 in the control arm and 152 in the study arm. Forty-eight patients in the control group and 15 patients in the study group were lost to follow-up. Patients were considered evaluable for study purposes if they received at least one phone call. Two hundred seventy-eight patients were included in the final analysis: 141 in the control group and 137 in the study group.
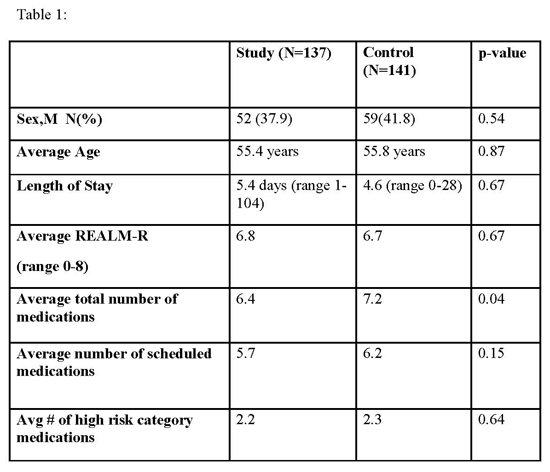
Demographic and disposition data for the control and intervention groups are shown in Table 1. The average length of stay for patients was 4.6 days for the control group and 5.4 days for the study group (p=0.67). The average REALM-R score for the control group was 6.7 compared to 6.8 in the study group (p=0.67). The primary reason for initial admission was infection in both the control (26.1%) and study group (26.3%).
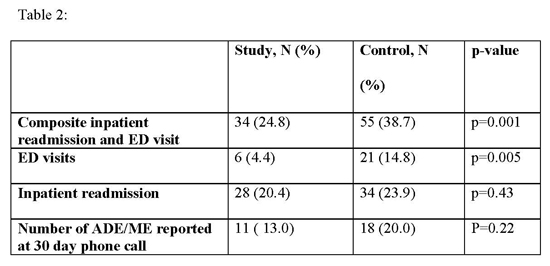
Of the 86 evaluable control patients, 18 patients experienced an ADE or ME, as compared to 11 out of 83 study patients (p=0.22). (Table 2).
The HCAHPS scores were assessed by the domain asking if a patient “clearly understood the purpose for taking each of their medications at the time of discharge.” This was analyzed by evaluating the two designated units six months prior to the start of the study in comparison to the six months of intervention period. The scores in the pre-study period showed 47% of patients surveyed chose “Agree” or “Strongly Agree” for the assessed domain. During the study period the HCAHPS score in this domain increased to 56%.
A total of 55 patients (38.7%) in the control arm experienced an inpatient readmission or ED visit within 30 days post-discharge compared to a total of 34 patients (24.8%) of the study arm (p=0.01). Of the patients who experienced an ED visit, 21 were enrolled in the control arm (14.8%) compared to 6 patients in the study arm (4.4%) (p=0.005). Inpatient readmissions were seen in 34 of the control patients (23.9%) compared to 28 of the study patients (20.4%) (p=0.43).
Discussion
While previous literature showed conflicting results regarding pharmacist impact on readmissions, our study demonstrated a decrease in the composite measure of inpatient readmissions and ER visits. The decrease in inpatient readmissions and ER visits could be attributed to multiple pharmacist interventions throughout the transitions of care. During medication reconciliation, 380 discrepancies were found in the study group compared to 205 in the control. Prior to discharge in the study group, pharmacist review of the discharge instructions identified discrepancies that were corrected prior to receipt by the patient, although this data was not quantified. All of the above mentioned interventions at different patient transitions through the healthcare system likely contributed to the lower rate of readmissions in the study group.
Characteristics of patients that were readmitted were evaluated and compared to non-readmitted patients in an attempt to provide insight into high-risk patients. A score of 6 or less is generally used to identify patients at risk for poor literacy. Although not statistically different, the REALM-R of readmitted patients in both study and control groups were numerically lower than non-readmitted patients. Likewise, the total number of medications in the readmitted groups was numerically greater than non-readmitted patients, but not statistically significant. No other factors assisted in discerning readmission risk.
While improvement in rate of ADE and MEs was demonstrated, the difference between the groups did not achieve statistical significance. Potential explanations include the subjective nature of ADE/MEs as well as a smaller than needed sample size to achieve sufficient power.
The increase in the HCAHPS scores relating to patient knowledge of medications at time of discharge may be attributed to pharmacist participation in the discharge process. Although the full impact of pharmacists’ intervention on this measure is unclear, the trend toward improvement is promising.
Compared with previous literature, our study design was unique in the number of phone calls made to patients post-discharge and in its prospective, randomized nature. In the previously mentioned study by Walker et al, phone calls were made only at days 3 and 30.6 Although the majority of our readmissions occurred within the first 14 days, by contacting patients twice within the critical 14 day period, we were potentially able to prevent additional readmissions. By contacting both the study and control group at 30 days, we were better able to assess the actual rate of readmission to all institutions, rather than just within our institution. Additionally, our study was distinct in the utilization of pharmacist extenders in the form of fourth year pharmacy students who were completing their advanced pharmacy practice rotation. Many institutions serve as training sites for students and residents, which provides an invaluable untapped resource to help provide exceptional transitional care.
Limitations to our study include exclusions due to the inability to educate prior to discharge, number of patients lost to follow-up at 30 days (primarily in the control group), the single center nature of the study and lack of complete readmission data from outside institutions.
Conclusion
Transitions of care is a high-risk situation for most patients and a multidisciplinary approach including pharmacists and pharmacy extenders may have a positive impact on reduction of prevention of ADEs/MEs, inpatient admissions, ED visits, and improvement in quality measures HCAHPS scores. The results of this study support the importance and impact pharmacist involvement has on measurable outcomes.
REFERENCES
- Gerhardt, G, Yemane A, Hickman P, Oelschlaeger A, Rollis E, Brennan N. "Data Shows Reduction in Medicare Hospital Readmissions in 2012." Medicare and Medicaid Research Research Review 2013; 3(2): E1-E11.
- Feigenbaum P et al. Factors contributing to all-cause 30-day readmissions: a structured case series across 18 hospitals. Med Care. 2012: 599-605.
- Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW. The incidence and severity of adverse events affecting patients following discharge from the hospital. Ann Intern Med. 2003; 138:161–7.
- Forster AJ, Murff HJ. Adverse Drug Events Occurring Following Hospital Discharge. J Gen Intern Med 2005; 20:317–323.
- Schipper JL, Kirwin JL, Cotugno MC et al. Role of Pharmacist Counseling in Preventing Adverse Events After Hospitalization. Arch Intern Med. 2006; 66:565-571.
- Walker PC, Bernstein SJ, Tucker Jones JN et al. Impact of Pharmacist-Facilitated Hospital Discharge Program. Arch Intern Med. 2009; 169:2003-2010.
Leadership Profile
Don Ferrill, PharmD
 What is your current leadership position in ICHP?
What is your current leadership position in ICHP? Champion
Where did you go to pharmacy school?
Creighton University School of Pharmacy and Allied Health Professions
Describe your current area of practice and practice setting.
I am currently the Pharmacy Education and Clinical Services Manager at Memorial Medical Center in Springfield, IL. I have worn several hats during the 22 years of service at Memorial including Pharmacy Supervisor, Operating Room Pharmacy Satellite Pharmacist, Anticoagulant Clinic Pharmacist, Pharmacokinetic Team Leader, IV Room Supervisor, and Staff Pharmacist.
What are you most proud of about your current role and practice setting?
The recent transformations of our pharmacy department, including increased utilization of robotic technologies that improve patient safety and allow our pharmacists to devote more time to clinical instead of distributive functions.
What initially motivated you to get involved, and what benefits do you see in being active in a professional association such as ICHP?
Personal professional development, networking and ultimately advancing our profession.
What advice would you give to pharmacists?
Never stop learning and get involved as much as you can as early as you can in your career.
Is there an individual you admire or look up to, or a mentor that has influenced your career?
Alisa Groesch, who is the Director of Pharmacy at Memorial Medical Center. She is extremely passionate about our pharmacy profession and is always learning and growing.
Do you have any special interests or hobbies outside of work?
Most of my spare time is spent with family, especially my wife and four children. We love to travel as much as possible. From 2005 to 2012, we took the camper all across the United States for extended summer vacations, visiting places like Yellowstone; Glacier National Park; Pike’s Peak; Rocky Mountain National Park; Niagara Falls; New York; Philadelphia; Washington, DC; Boston; Bar Harbor, Maine; and as far as the Grand Canyon and Southern California.
What is the most interesting/unique fact about yourself that few people know?
My four children’s ages have a wide range – from 27 years old to 15 months.
What is your favorite quote?
“I’m not young enough to know everything” -Oscar Wilde
The GAS From Springfield
The 2014 Election
by Jim Owen and Scott Meyers
The campaign season is upon us…as if you have not been able to tell from the incessant advertisements on television, radio and in the mailboxes. This year’s election will go down in the history books for a lot of reasons, most of which will not be good. We hope to provide a brief look at the state elections and where we think the elections and our organization will be in January after the dust has settled.
The Illinois House of Representatives
All 118 seats of the House of Representatives are up for election this year. Of the 118 seats only 50 districts have two or more candidates in the general election. The other 68 seats have candidates who have no opponent. Of the 50 seats where there are opponents, 41 seats have an incumbent representative in place that is running for reelection. There are 9 seats that are open and not represented by an incumbent. The retention rate in Illinois for incumbents in the House and Senate is very high – in excess of 95%. Just looking at the seats that are up it appears that the Illinois House will continue to be controlled by Democrats and that Speaker Madigan will continue as Speaker.
The Illinois Senate
Of the 59 seats in the Illinois Senate, only 19 are up for election this cycle. Of the 19 seats up for election, only 7 seats have a challenger for the incumbent State Senator. It is doubtful that there will be any change in the composition of the State Senate after this election. The Democrats will maintain their majority and President Cullerton will remain in control.
The Race for Governor
Incumbent Governor Pat Quinn and his opponent Bruce Rauner will undoubtedly set records this year in Illinois history.
First, this race will go down as the most negative statewide race in Illinois. Both campaigns have focused on the other candidates perceived weaknesses and not campaigned on their own policies. You ask why? The biggest part of modern election strategy is to make the voter not want to vote for the other guy. Unfortunately, as negative as this campaign has been, a lot of people will choose not to vote at all. That is why there is a lot of speculation that this could be a record low turnout in the percentage of voters going to the polls.
Second, this race will go down as the most expensive statewide race on the record books. We would not be surprised to see the total spent in excess of $70 million by the time the votes are counted. Imagine that, with a total turnout of approximately 3.2 million voters that’s $22 for every vote cast and we are probably light on the estimated expenditures.
At the time of this writing, this election is too close to predict. The only thing predictable is that with three weeks to go until Election Day, we will see a lot more commercials, and if it ends up like the last election, a few thousand votes will separate the winner from the loser. With Illinois’ many problems, we wish the victor well. We hope whoever wins has the ability to put the state on a better track and can do so in a bipartisan manner. Great challenges are ahead for our next Governor.
Please cast your ballot on November 4.
College Connections
Mental Health Awareness
by Neha Kapur, P3, UIC-Rockford Student Chapter President
“I felt alone, because I was trying to hide what was happening to me from my family and friends. I was depressed, angry, embarrassed and ashamed because I couldn’t cope. I was exhausted from all my self-punishment and the frequency and severity of the anxiety attacks. I had no quality of life - enough was enough.”
The above statement was written in “My Mental Health Journey: From Anxiety to Rehabilitation,” a personal story by a woman named Tish. Tish, like many other individuals, has been struggling with mental illness and feels embarrassed by her disease and inability to cope with her thoughts and feelings independently. Due to experiences like Tish’s, UIC’s ICHP chapter has put forth its best effort to reduce the stigma surrounding mental illness and bring awareness to the struggles of patients and family members. Additionally, we have worked hard to promote mental wellness for individuals without mental illnesses.
In order to expand our mental health initiative, ICHP has worked closely with the National Alliance on Mental Illness (NAMI). One of the ways our chapter has collaborated with the organization is by inviting patients who had difficulty overcoming their mental disorders, to come speak to students. By listening to their stories and interacting with them on a personal level, we were able dismiss many of the misinformed judgments and opinions commonly made about mental illness topics. Armed with an improved understanding of their issues, students are better prepared to provide care for our patients.
Furthermore, our chapter has been involved with NAMI by scheduling support group visits for students to attend. At the SwedishAmerican Hospital in Rockford, NAMI holds bi-monthly meetings where family members, friends and caregivers of individuals living with a mental illness gather to discuss their personal struggles in caring for someone with a mental disorder. It is a great way for students to gain a new understanding of mental illness. Some of the information the support group has shared with students is failed therapies, the repeating behavioral cycles of their loved ones and emotional distress. Needless to say, it has been an eye-opening experience as many times health care providers focus their attention on the patient rather than the caregiver, who may also need supportive therapy.
Aside from NAMI, ICHP has also held some events on campus to help lift students’ spirits and promote mental prosperity. As an annual event during finals week, ICHP invites Caring Canines to bring their dogs to school to play with the students. This has been a successful event as it provides students with a much needed stress-relieving break. Additionally, we have created and distributed finals week packages to students during final exams. Again, this is our way of encouraging students to make the effort to evaluate their mental status and find ways to reduce their mental burden, even if it is as simple as buying a small care package.
Because of all of the effort ICHP has put toward bringing awareness to mental health issues and wellness, I am extremely grateful to be an active member. I feel as though I am learning more about the issues regarding the various diseases and helping give patients and caregivers a voice to future health care professionals. I look forward to further expanding our mental health initiative by bringing more awareness to the community.
American Pharmacists Month at Rosalind Franklin University
by Amanda Outinen, P3, Student Chapter President, Rosalind Franklin University of Medicine & Science College of Pharmacy
American Pharmacists Month is celebrated and promoted during the entire month of October. At Rosalind Franklin University, the month is filled with events including speakers, campus and community outreach, competitions, and a college spirit day. The spirit day encourages students to wear their pharmacy organization or college of pharmacy clothing to promote the pharmacist’s role in patient care to the rest of the community.
Each pharmacy organization and class student council hosts a speaker during the month. Our ICHP-SSHP chapter hosted Dr. Diana Isaacs, the 2014 recipient of the ICHP New Practitioner Leadership Award, who spoke on getting involved and becoming a standout candidate. These lunchtime speakers motivate the students, provide additional learning opportunities, and allow our students to network with current pharmacists. The presentations sponsored by our pharmacy organizations and lead by pharmacists allow for our students to receive life-long learning credit. Life-long learning credits are required by our college. Students attend pharmacy presentations outside of class and submit a reflection on the presentation to receive credit. Life-long learning prepares our students for completing continuing education credits once they are pharmacists.
Another annual event during American Pharmacists Month on our campus involves our pharmacy students running an influenza immunization clinic on campus. The student chapter of APhA organizes the immunization clinic, but all pharmacy students are welcome to volunteer their time and practice their immunization skills. Immunization certification occurs during the first year at our college, so all students are able to participate in providing immunizations at this event. The first year students especially enjoy volunteering their time at the immunization clinic since they are eager to practice their new skills.
Our students also reach out to the university campus and surrounding community to educate people on the variety of services that pharmacists can offer by setting up booths with information and games. To motivate our pharmacy students the college hosts a “Quest for the Best: Pharmathon” consisting of fun games based on pharmacy knowledge. Pharmacy faculty and staff run the games, and prizes are awarded to the winners at the end of the competition.
The ASHP Clinical Skills Competition, one of the highlights of the month, is hosted by our ICHP-SSHP chapter at the end of October. Students look forward to practicing their clinical skills and competing for the chance to advance to the national competition held during the ASHP Midyear Clinical Meeting. American Pharmacists Month is a busy time at Rosalind Franklin University College of Pharmacy and keeps our students active and involved in promoting pharmacy and learning about pharmacy practice outside of the classroom.
Life on an Indian Reservation: APPE Edition
by Ashley Brown, P4, Midwestern University Chicago College of Pharmacy
 The Navajo people tie their culture into their everyday lives in any way possible. This was apparent when I first entered the Tsehootsooi Medical Center on my first day through a revolving door that turned clockwise. I learned that the Navajo people believe life moves in a clockwise direction and thus, their revolving doors do the same. This was one example of how the Navajo people keep their culture alive.
The Navajo people tie their culture into their everyday lives in any way possible. This was apparent when I first entered the Tsehootsooi Medical Center on my first day through a revolving door that turned clockwise. I learned that the Navajo people believe life moves in a clockwise direction and thus, their revolving doors do the same. This was one example of how the Navajo people keep their culture alive.
This was my first advanced pharmacy practice experience (APPE) and it was located on a Navajo Indian reservation in Fort Defiance, Arizona. I jumped into the rotation immediately counseling Navajo patients using the comprehensive Indian Health Service (IHS) counseling techniques. The patients were kind and accommodating as I learned alongside pharmacists and physicians. I quickly grasped the questions not to ask patients about their culture, specifically regarding rituals or components of their herbal teas. The patients were open to sharing their Navajo beliefs, but some parts remained private. I had the opportunity to work beside emergency room physicians, surgeons, primary care doctors, nurse anesthetists, and U.S Army Special Forces medics which all helped to broaden my knowledge.
The hospital includes a diabetes clinic, asthma clinic, primary care clinic, tuberculosis clinic, anticoagulation, optometry, dentistry, respiratory therapy, and physical therapy. I was shown how interdisciplinary teams efficiently work together and support their patients, both inpatient as well as outpatient. I immersed myself in the common disease states seen on the reservation such as diabetes, hypertension, and hyperlipidemia, both clinically and actively. The community organized several 5K races throughout the summer and I had the opportunity to run a 5K alongside the community members. It was motivating to be apart of the proactive choices the community was making to better their health and increase health awareness. I was also given the opportunity to teach a lecture on medication administration at a nearby school for staff members who were the caretakers of students living in the dormitories. Our lecture covered hand washing to Tylenol dosing to treating impetigo. It was rewarding to learn inside and outside of the hospital, while participating in community life.
There were many challenges on the reservation that I had never been exposed to before. Many patients hitchhiked their way to the hospital or walked long distances, since they had no access to transportation. Others did not have electricity to store their insulin products. My projects reflected these issues, such as creating a reference sheet for healthcare professionals so they could instruct patients when each of their insulin products expired without refrigeration.
The time I spent outside of the hospital was rich in culture. I attended an inter-tribal ceremony and was invited into the homes of natives for their summertime feasts. However, the compassion felt by the doctors around me was the highlight. I worked with doctors that were passionate about their work and treated the patients with respect, care, and a gentle demeanor. The site reignited my enthusiasm for pharmacy, while putting me outside of my comfort zone to help develop me into a well-rounded healthcare professional.
More
Officers and Board of Directors
LINDA FRED
President
GINGER ERTEL
Treasurer
660-342-5022
gertel@msn.com
CHARLENE HOPE
Secretary
773-292-8200 x4190
TRAVIS HUNERDOSSE
Director, Educational Affairs
thunerdo@nmh.org
CARRIE VOGLER
Director, Marketing Affairs
217-545-5394
DESI KOTIS
Director, Professional Affairs
KATHRYN SCHULTZ
Director, Government Affairs
312-926-6961
MIKE WEAVER
Chairman, House of Delegates
815-599-6113
mweaver@fhn.org
ANA FERNANDEZ
Technician Representative
DAVID TJHIO
Chairman, Committee on Technology
816-885-4649
david.tjhio@cerner.com
BRANDI STRADER
Chairman, New Practitioners Network
217-544-6464
JACOB GETTIG
Editor & Chairman, KeePosted Committee
630-515-7324 fax: 630-515-6958
jgetti@midwestern.edu
SCOTT MEYERS
Executive Vice President, ICHP Office
815-227-9292
scottm@ichpnet.org
Regional Directors
KATHRYN SCHULTZ
Regional Director North
JULIA SAPOZHNIKOV
Student Chapter Liaison
University of IL C.O.P.
sapozhn1@uic.edu
NEHA KAPUR
President, Rockford Student Chapter
University of IL C.O.P.
kapur4@uic.edu
CAROLYN TOY
President, Student ChapterMidwestern University C.O.P.
ctoy59@midwestern.edu
MARIA LAURA ITUAH
President, Student Chapter
Chicago State University C.O.P.
mituah@csu.edu
KIMBERLEE KABBES
President, Student Chapter
Southern Illinois University Edwardsville S.O.P
kikabbe@siue.edu
COURTNEY MAKOWSKI
President, Student Chapter
Roosevelt University C.O.P.
JULIA SCHIMMELPFENNIG
President, Metro East Society (MESHP)
jschimmelpfen@sebh.org
MEGAN METZKE
President, Sangamiss Society
memiller8@yahoo.com
ED RAINVILLE
President, West Central Society (WSHP)
309-655-7331x
ed.c.rainville@osfhealthcare.org
Vacant Roles at Affiliates —
President, Rock Valley Society; Southern IL Society; Sugar Creek Society; Regional Director, South
Welcome New Members!

| New Member |
Recruiter |
|
|
| Lisa Nguyen |
|
| Brittany Lee |
|
| Mallory Adams |
|
| Susan Nichols |
|
| Tony Tran |
|
| Joanna Wojtyczka |
|
| Katarzyna Plis |
|
| Ashley Kral |
Ann Corkery |
| Sang Wan Kim |
|
| John Littler |
|
| Danya Faruqi |
|
| Hankyung Cho |
|
| Rakhshan Naseeb |
|
| Mollie Roark |
|
| Matthew Horney |
|
| Sara Gubala |
|
| Yun Jee Jeong |
|
| Rina Patel |
|
| Sandy Ezzet |
|
| Nabiha Sabiri |
|
| Trevor Luman |
|
| An Nguyen |
|
| Bradley Killmer |
|
| Patrice Davis |
|
| Kevin Heath |
|
| Logan Osborn |
|
| Nisaa Rattani |
|
| Michael Bailey |
|
| Jared Lang |
|
| Lance Rodriguez |
|
| Xing Jin |
|
| Yi-Hsuan Huang |
|
| Angelico Fernandez |
|
| Samantha Wheeler |
|
| Sergey Brevda |
|
| Kati Stegner |
|
| Manar Kandil |
|
| Green Kristi |
|
| Cheryl Pitts-Williamson |
|
| Shane Murphy |
|
| Irene Park |
|
| Brandon Barringer |
|
| Michael Ranzini |
|
| Hiral Patel |
|
| Jason Williamson |
|
| Christen Parks |
|
ICHP Pharmacy Action Fund (PAC) Contributors
Names below reflect donations between November 1, 2013 and November 1, 2014. Giving categories reflect each person's cumulative donations since inception.
ADVOCACY ALLIANCE - $2500-$10000 Kevin Colgan
Edward Donnelly
Dave Hicks
Frank Kokaisl
Michael Novario
LINCOLN LEAGUE - $1000-$2499
Scott Bergman
Andrew Donnelly
Ginger Ertel
Linda Fred
James Owen Consulting Inc.
Jan Keresztes
Kathy Komperda
Despina Kotis
William McEvoy
Scott Meyers
Michael Rajski
Edward Rickert
Christina Rivers
Michael Short
Carrie Sincak
Miriam Mobley-Smith
Avery Spunt
Michael Weaver
Patricia Wegner
Thomas Westerkamp
CAPITOL CLUB - $500-$999 Sheila Allen
Margaret Allen
Rauf Dalal
Drury Lane Theater
Ann Jankiewicz
Leonard Kosiba
George MacKinnon
Janette Mark
Mary Lynn Moody
Edward Rainville
JoAnn Stubbings
UIC Student Chapter
Jill Warszalek
GENERAL ASSEMBLY GUILD - $250-$499 Tom Allen
Pete Antonopoulos
Peggy Bickham
Jaime Borkowski
Sandra Durley
Nancy Fjortoft
Michael Fotis
Travis Hunerdosse
Zahra Khudeira
Ann Kuchta
Mary Lee
Gloria Meredith
Jennifer Phillips
Justin Schneider
Kathryn Schultz
Heidi Sunday
Alan Weinstein
SPRINGFIELD SOCIETY - $100-$249 Jen Arnoldi
Jerry Bauman
Jill Borchert
Donna Clay
Mark Deaton
John Esterly
Gireesh Gupchup
Joann Haley
Joan Hardman
Charlene Hope
Diana Isaacs
Kim Janicek
Stan Kent
Kati Kwasiborski
Kristopher Leja
Ronald Miller
New Practitioners Network
Karen Nordstrom
Peggy Reed
Katie Ronald
Brandi Strader
Jennifer Tryon
Carrie Vogler
Marie Williams
William Wuller
Cindy Wuller
GRASSROOTS GANG - $50-$99
Brett Barker
Susan Berg
Jeanne Durley
Mary Eilers
Lara Ellinger
Clara Gary
Tory Gunderson
Carol Heunisch
Brian Hoff
Robert Hoy
Mike Koronkowski
Kim Lim
Mark Luer
Bella Maningat
Milena McLaughlin
Megan Metzke
Katherine Miller
Mark Ruscin
Stacy Schmittling
Evanna Shopoff
Lucas Stoller
Jerry Storm
Dave Willman
Janeen Winneke
Amanda Wolff
CONTRIBUTOR - $1-$49
Renee Advincula
Yinka Alaka
Lisa Ball
Roger Ball
Marci Batsakis
Greg Biedron
Amy Boblitt
John Chaney
Kathy Cimakasky
Mardhia Dayisi
Andreea Ducu
Veronica Flores
Deb Fox
Janice Frueh
Crystin Gloude
Linda Grider
Alisa Groesch
Rebekah Hanson
Margaret Heger
Ina Henderson
Julie Kasap
Dijana Keljalic
Nehrin Khamo
Josephine Kochou
Huda-Marie Kuttab
Irvin Laubscher
Chris Little
Kristopher Lozanovski
Laura Mazzone
Kit Moy
Syed Munawer
Whitney Palecek
Hina Patel
Abby Reeder
Cheryl Scantlen
Elba Sertuche
Hannah Sheley
Chris Shoemaker
Carrie Silverman
Theophilus Simon
Jennifer Splawski
Gloria Sporleder
David Tjhio
Zakarri Vinson
Michael Wilcox
Christina Yates
Thomas Yu
Upcoming Events

Tuesday, November 4 at 3:00pm & Thursday, November 13 at 12:00pm
Champion Webinar: Drug Choice and Dosing in the Patient with Advanced Liver Disease
LIVE Webinar
Tuesday, November 18th, 2014 at 5:00-7:00pm
CPE Event! Description HMG-CoA Reductase Inhibitors and the Risk of Diabetes Mellitus
American Harvest Eatery | Springfield, IL
Thursday, November 20th, 2014 at 6:30-8:00pm
CPE Event! Description What’s So Special About Specialty Pharmacies? Overview and Role of Pharmacists and Pharmacy Technicians
University of Illinois at Chicago College of Pharmacy | Chicago, IL
Monday, December 8
Illinois Reception at the Midyear
Anaheim Hilton, Ballroom D | Anaheim, CA

Print Entire Issue