Print Entire Issue
New Practitioners Network

KeePosted Info
Features
Register Now!
Meet the 2014 ICHP Student Pharmacist Intern
It's Back! The Auction With a Twist
Columns
President's Message
Directly Speaking
Medication Safety Pearl
New Practitioners Network
The GAS From Springfield
College Connections
Cultivating Communication
Pura Vida
A Student Pharmacist’s Introduction to MTM
More
Officers and Board of Directors
Welcome New Members!
ICHP Pharmacy Action Fund (PAC) Contributors
Upcoming Events
KeePosted Info
 Illinois Council of Health-System Pharmacists
Illinois Council of Health-System Pharmacists
4055 North Perryville Road
Loves Park, IL 61111-8653
Phone: (815) 227-9292
Fax: (815) 227-9294
www.ichpnet.org
KeePosted
Official Newsjournal of the Illinois Council of Health-System Pharmacists
EDITOR
Jacob Gettig
ASSISTANT EDITOR
Jennifer Phillips
MANAGING EDITOR
Scott Meyers
ASSISTANT MANAGING EDITOR
Trish Wegner
DESIGN EDITOR
Amanda Wolff
ICHP Staff
EXECUTIVE VICE PRESIDENT
Scott Meyers
VICE PRESIDENT - PROFESSIONAL SERVICES
Trish Wegner
DIRECTOR OF OPERATIONS
Maggie Allen
INFORMATION SPECIALIST
Heidi Sunday
CUSTOMER SERVICE AND
PHARMACY TECH TOPICS™ SPECIALIST
Jo Ann Haley
ACCOUNTANT
Jan Mark
COMMUNICATIONS MANAGER
Amanda Wolff
LEGISLATIVE CONSULTANT
Jim Owen
ICHP Mission Statement
Advancing Excellence in the Practice of Pharmacy
ICHP Vision Statement
ICHP dedicates itself to achieving a vision of pharmacy practice where:
- Pharmacists are universally recognized as health care professionals and essential providers of health care services.
- Patients are aware of the training, skills, and abilities of a pharmacist and the fundamental role that pharmacists play in optimizing medication therapy.
- Formally educated, appropriately trained, and PTCB certified pharmacy technicians manage the medication distribution process with appropriate pharmacist oversight.
- Pharmacists improve patient care and medication safety through the development of effective public policies by interacting and collaborating with patients, other health care professionals and their respective professional societies, government agencies, employers and other concerned parties.
- Evidence-based practices are used to achieve safe and effective medication therapies.
- There are an adequate number of qualified pharmacy leaders within the pharmacy profession.
- Pharmacists take primary responsibility for educating pharmacy technicians, pharmacy students, pharmacist peers, other health professionals, and patients about appropriate medication use.
KeePosted Vision
As an integral publication of the Illinois Council of Health-System Pharmacists, the KeePosted newsjournal will reflect its mission and goals. In conjunction with those goals, KeePosted will provide timely information that meets the changing professional and personal needs of Illinois pharmacists and technicians, and maintain high publication standards.
KeePosted is an official publication of, and is copyrighted by, the Illinois Council of Health-System Pharmacists (ICHP). KeePosted is published 10 times a year. ICHP members received KeePosted as a member benefit. All articles published herein represent the opinions of the authors and do not reflect the policy of the ICHP or the authors’ institutions unless specified. Advertising inquiries can be directed to ICHP office at the address listed above. Image disclaimer: The image used in the Pharmacy Tech Topics advertisement is the property of © 2014 Thinkstock, a division of Getty Images.
Copyright © 2014, Illinois Council of Health-System Pharmacists. All rights reserved.
Features
Register Now!
Join Us in Charting a Bold Course for Illinois Pharmacy!
What does the word “bold” mean to you? The Merriam-Webster dictionary defines it as “not afraid of danger or difficult situations,” or “showing or needing confidence or lack of fear.”1 ICHP President, Michael Fotis, selected “bold” as his presidential theme because he felt that it is “A Time to be Bold” in pharmacy. Here are some excerpts from his
presidential address. “…Our nation is working to transform healthcare and pharmacists need to work to transform the practice of pharmacy. In order for us to formulate new directions, new ways of doing things we must have our own knowledge and understanding of every key issue, not simply repeat what is taught….Our healthcare system does not always work very well…there are too many avoidable errors, much cost inefficiency, and for the most part we leave our most vulnerable patients to fend for themselves. So many pharmacists [and technicians] do exceptional work to improve our health system. We need to change the way we work as pharmacists [and technicians] so that all of us can provide this level of care. Our patients need us to do this.” Mike’s advice to all of us, especially students, is:
- Learn when and how to ask questions;
- Learn when and how to set goals;
- Work with your mentors to determine if our activities are worth doing;
- Have interests beyond a single area of expertise;
- Help [pharmacy] to formulate new directions, new ways of doing things by having your own knowledge and understanding
This year’s Annual Meeting will be Charting a Bold Course for Illinois Pharmacy through the provision of continuing education programming in clinical, management, technology, pharmacy practice, technician and student areas of interest where we can take bold steps in advancing pharmacy practice. We are thrilled to have Rita Shane, a keynote speaker known for her bold approach to patient care.
Sharing bold ideas and initiatives will be possible through networking opportunities at the Annual Meeting. Join us at the Town Hall where you have a chance to speak up about ICHP and its services; visit our partner vendors at the Exhibit Program; visit with residency program directors at the Residency Showcase; and engage with fellow colleagues.
Are you ready to hoist the sails and chart a bold new course for patient care?
Reference:
Meet the 2014 ICHP Student Pharmacist Intern
by Kelly Delehanty, P3, University of Illinois College of Pharmacy at Rockford
 Hi, my name is Kelly Rose Delehanty and I am the Illinois Council of Health-system Pharmacists pharmacy student summer intern. I grew up in Loves Park, IL, which is five minutes away from ICHP headquarters. Since the age of three, my extracurricular activities focused on dance lessons, recitals, and competitions. I have studied varying types of dance including ballet, tap, jazz, Irish and traditional Italian. Besides dancing, I am an avid reader and creative writer. After graduating from high school in 2008, I attended Western Illinois University where I received my Bachelor of Science degree in Biochemistry in 2012.
Hi, my name is Kelly Rose Delehanty and I am the Illinois Council of Health-system Pharmacists pharmacy student summer intern. I grew up in Loves Park, IL, which is five minutes away from ICHP headquarters. Since the age of three, my extracurricular activities focused on dance lessons, recitals, and competitions. I have studied varying types of dance including ballet, tap, jazz, Irish and traditional Italian. Besides dancing, I am an avid reader and creative writer. After graduating from high school in 2008, I attended Western Illinois University where I received my Bachelor of Science degree in Biochemistry in 2012.
While attending Western Illinois University, I was involved in student organizations. The fall of my freshman year I rushed the Delta Zeta sorority. Joining a sorority instilled a sense of teamwork and loyalty which I hope will transfer over into my future pharmacy career. I also worked as a Resident Assistant for my last two years at Western. As an RA, I was presented with the opportunity to develop my leadership abilities. I always knew I wanted to be a pharmacist, so when I was accepted to the University of Illinois College of Pharmacy in my home town I was elated.
As I enter my third year of pharmacy school, I am realizing just how quickly time is passing. This year I will serve as President of Phi Lambda Sigma, Vice Regent of the Epsilon Rho chapter of Kappa Psi pharmaceutical fraternity and Vice President of Fundraising for APhA-ASP. To say I will be busy is an understatement, but I enjoy the constant activity of submersing myself in the profession of pharmacy.
My summer project as the ICHP pharmacy student intern involves updating the key contact list for the Health-System Pharmacy Response Network. This response network will be used during emergencies in the state of Illinois. To test the emergency response system, I will conduct a practice drill requesting the quantity of a specific medication. The pharmacy will be provided with the name, strength, and dosage form of the medication via fax or email. After all the data has been collected, I will analyze the results categorizing the data by response time, region of the pharmacy, and quantity of medication on hand at the time of the drill.
I look forward to the rest of my time at ICHP working with the amazingly supportive staff of Scott, Jan, Maggie, Trish, Jo, Heidi, and Amanda.
It's Back! The Auction With a Twist
by Scott A. Meyers, Executive Vice President
Summer is almost here! Before we know it, the ICHP Annual Meeting will be here too and the return of the ICHP Pharmacy Action Fund “Auction With A Twist”.
You may remember that the “Auction With A Twist” is a fun and exciting way to raise money for ICHP’s Advocacy efforts, and for the numerous winners, a great way to score some big prizes! After a rest last year as we celebrated the ICHP Golden Anniversary, it is back by popular demand for the 2014 ICHP Annual Meeting on September 11-13 at Drury Lane Theater in Oakbrook Terrace, Illinois.
And now it’s time to start planning, purchasing or preparing the prize you and your colleagues want to donate to this year’s Auction. Two years ago the iPad, iPod, iPod nano, Kindle, Nook, flat screen TV, golf clubs, wines, sports tickets and College of Pharmacy memorabilia were all hot properties! This year it could be any of these things and more, but it’s really up to all of you! Get a team together and contribute a gift you would love to win yourself!
And remember, as ICHP members, you don’t even have to attend the Annual Meeting to bid on and win the prizes! The online auction occurs the two weeks prior to the Annual Meeting and with our “Auction With A Twist” format, you have the same chance of winning. Visit the ICHP website to learn more about the fun and excitement in store for all this fall.
So get your colleagues together and start planning what big prize you’re going to contribute or send us something with your personal touch to be auctioned off at the 4th Annual “Auction With A Twist!”
The deadline for prize donations is August 1st. If you have a prize you would like to donate, please email Scott Meyers at ScottM@ichpnet.org or call the office at 815-227-9292.
And don't forget about the $1K Raffle
Help the ICHP Pharmacy Action Fund meet its 2014 fundraising goal of $25,000 this year and at the same time perhaps win a cool $1,000. The Pharmacy Action Fund, ICHP's political action committee, is asking every pharmacist member to contribute at least $25 and every student and pharmacy technician to add their own $5 contribution before this fall's elections. The $1K Raffle is just one of three major fund raisers this year but definitely the one with the biggest potential payoff!
Members may purchase raffle tickets beginning on February 1, 2014 until 11:30 a.m. on September 13, 2014 at the ICHP Annual Meeting to obtain a chance at the $1,000 prize. For more information and to purchase raffle tickets, please click to download the $1K Raffle Form.
Contributions to the ICHP Pharmacy Action Fund are not considered charitable contributions by the IRS.
Columns
 President's Message
President's Message
Your First Job as a Pharmacist
by Mike Fotis, ICHP President
Whether you are fresh out of school or have just completed your residency, your first job as a pharmacist will have a major impact on the type of career you have. What should you look for?
Your first step is to take a few moments to reflect on your own professional values. Answering the following questions should give you a good start. What sort of pharmacist do you plan to become? What will you stand for? Try writing your own professional practice statement. It is difficult to identify the positions that are right for you until you have carefully thought about your own personal goals. We all want to work with colleagues who share common purpose, motivations and values.
How can you tell the type of candidate a pharmacy leader is looking for? I suggest you take a close look at the recently hired pharmacists. Of course, this assumes you have the opportunity to meet with them. (By the way, ICHP meetings are a great place to do this!) Are the recent pharmacists enthusiastic about their position? Or is speaking with you about their positions a chore to them? What are their professional values? Are they similar to yours? If you share professional values with future colleagues, there is a very good chance that department is a good fit for you.
Meet with departmental leadership and assess their goals for pharmacy. First off, are you having a two way conversation or a one way conversation? If the conversation is one way, meaning you do not get an opportunity to express your opinions to someone who is listening to you, think about this for a long time. What about the practice of pharmacy? Does the leader plan to push the envelope or are they content to maintain the status quo? At first, maintaining the status quo seems to be the safest option, but is that really true? How safe is the status quo? If you are starting out in your career, you are going to practice for 25 to 30 years or more. Do you really think maintaining the status quo is the safe approach?
Ask about the ASHP Pharmacy Practice Model Initiative (PPMI). Departmental leadership should fully support this initiative. Full support means they subscribe to the principles that a) every patient deserves a pharmacist and b) the pharmacist is first responsible to the patient. Our goal should be to protect our patients, not to just protect our jobs.
In order to achieve the goals of the PPMI, the department needs to be committed to an all hands on deck approach. Take an assessment of all pharmacy technicians, pharmacy students, pharmacy residents, and new practitioners. Is there a plan so that in the near future every one of these groups will be working at the top of their skill set?
What can YOU do about it? Develop a plan for continuing professional development (CPD). Can you build a few minutes for professional development into your daily activities? The reality is that pharmacy practice is fast paced. You will be drained by the end of the day. Your plan for CPD has to be a part of your daily routine.
Get involved right now. Play an active role in a forward thinking professional organization like ICHP and ASHP. Develop your confidence, learn new ways of doing things and build a professional network of clinicians who share your ideals and goals. We are in a tough economy, and it can be challenging to find a job of any kind. Taking some extra time to find a job that is a good fit for your professional goals means that you have to be bold. It won't be easy, but are there many worthwhile things that are easy?
 Directly Speaking
Directly Speaking
Transition of Care: A View from the Other Side
by Scott A. Meyers, Executive Vice President
Transition of care is not a new term – it’s been around for many years. It’s not a catch phrase, buzzwords or marketing term. It is something we’ve been talking about for a long time and unfortunately that’s about all. I think part of the problem could be that we don’t appreciate the real meaning until we’ve lived it from the other side.
Well in the two short months of nice weather we’ve had this year, I’ve lived it on the other side with two different family members. Both entered the hospital through the emergency department of their respective hospitals. One because it was a true emergency and the other because the primary care physician involved did not have admitting privileges. The latter, taking two attempts for admission with what turned out to be a nasty case of C. Diff!
Both family members spent about a week in the hospital and then both, who were elderly and severely compromised by their initial problems, ended up in two different nursing homes to rehab before going home. In the case of the patient with C.Diff., there was good communication in advance, and the nursing home was prepared with the necessary doses of vancomycin. However, medications for GERD, sleep and anxiety were not there at the onset, and at least one day was lost for each. The other patient, who went home without antibiotics did, however, have to wait a full day for diabetes, blood pressure and pain medications.
In all the above mentioned cases, life and death was not imminently in the balance, but certainly missing a couple of doses of vancomycin could lead to resistance and additional unnecessary treatments. In addition, the medication reconciliation process from hospital to nursing home was less than desirable. The patient with blood pressure medications was sent to the nursing home on a different regime than he had been on at home, and to be honest, it was probably better than what he had been taking prior to admission.
Which brings me back to the hospital admission transition. When admitted, the patient was NPO for several days and because of that, no meds were administered. When the patient returned from surgery and was experiencing significantly elevated blood pressure, there were no orders for any meds and more importantly any records of the previous regime. Seems to me that that transition wasn’t very smooth either.
These experiences have left me with a new appreciation of the hurdles the regular patient and their family have to face when navigating our health care system. Care is fragmented, communications are poor at best even within the hospital or the nursing home. Without a strong understanding of the processes and their intricacies, patients and their families are lost…wandering through a system that has so much to offer but does a really bad job of coordinating it.
Is it because we have become so “siloed”, or are we too focused on our particular part? These problems may not occur in every hospital with every transition, but I’m sure they happen much more often than we see. And in many cases, no one even realizes that it’s happening.
I believe it is time to review and revise our current transition processes. At a recent Clinical Specialist and Research Network meeting, this was a topic of discussion. There, the presenter asked hospital pharmacists in the group to encourage their administrators to allow the supply of 24 hours of medications to patients at the time of discharge to a nursing home. This would allow ample time for the nursing home pharmacy to provide the needed medications. The problem with this request is that most third party insurers won’t pay for those medications. So working within the hospitals and nursing homes will not solve the problem by itself. But the discussions must escalate to a level that brings in all involved parties.
We need to make sure that medication reconciliation is done efficiently and effectively at both ends of the stays and work to provide solid discharge planning and counseling. These processes may not even be in the circle of influence of some pharmacy departments, but they should be. The pharmacy department should work with discharge planners and the nursing home pharmacy providers and reach out to insurers to convince them to reimburse for the 24-hour supply for transfer patients. That way, no patient goes without needed medications when they leave our facilities. We need to look at these transitions of care from the patient’s side just to make sure we’re not missing anything. It looks a lot different from there!
Medication Safety Pearl
Implementation of an Electronic Profile Card for Chemotherapy Preparation
by Sarah Engberg, PharmD, OSF Saint Francis Medical Center, Peoria, IL
Children’s Hospital of Illinois is a pediatric hospital within OSF Saint Francis Medical Center in Peoria, Illinois. It is a full service tertiary hospital with 127 beds, more than 115 pediatric specialists, and 40 pediatric sub-specialties. The hospital has also served as the location for the St. Jude Midwest Affiliate Clinic since 2002.
Institution policy required a pharmacist to hand write preparation instructions on an IV profile card prior to compounding of chemotherapy. This information was obtained from our institution IV guidelines for hazardous medications or per the manufacturer package insert. A copy of the prescription label was placed on the front of the card while the back of the profile contained space for documentation of duration, stability, storage requirements, special instructions (Do Not Tube, Hazardous, etc.), and required auxiliary labels (Chemo/Hazardous, Intrathecal Use Only, etc.). A second pharmacist would then provide an independent double check of the profile to ensure all of the information was correct. Date, time, compounding technician/pharmacist, and verifying pharmacist were all documented on the back of the IV profile card. This procedure contained several opportunities for errors – human errors in transcribing instructions to paper, legibility of handwriting, inappropriate box selection, and math errors resulting in incorrect volumes and concentrations.
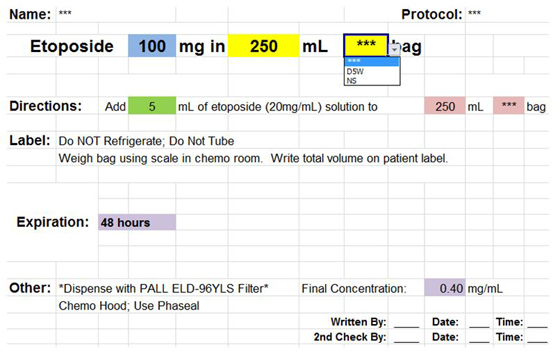
In 2011, OSF St. Francis Medical Center Children’s Hospital of Illinois initiated a new policy involving the creation of electronic IV profile cards for inpatient use and repeated outpatient use. For inpatient use, an IV profile card is used one time and then filed away in storage. IV profile cards for outpatients are used multiple times, as the patient comes back several times within their chemotherapy cycle and receives the same dose of chemotherapy. Documentation areas in each of the respected profiles were customized to fit the needs of the population. Inpatient profile cards contained an area to place the preparation label for IV compounding as well as a chart to write the date and time made and initials of the compounding technician and verifying pharmacist. In addition to the previous mentioned documentation, the outpatient IV profile cards contained additional areas in the chart to document the patient specific hospital number, the specific order number of the chemotherapy, and the week in their chemotherapy protocol. These areas allow the profile to be used multiple times while still identifying the specific compounding information. The remainder of the sections (medication name, dose, and diluent; directions; labels required; expiration; other) were consistent between profiles. The electronic profile was created utilizing the hospital’s current IV guidelines for preparation of hazardous medications. Most of the IV profile card is locked from editing to avoid errors due to alteration of information. Preparation instructions, storage, random needed information (such as special filters to send), and label requirements are all pre-written and locked from editing. The only area available to manually type information is the dose of medication (blue box in Figure 1). Drop down boxes are available to select a specified bag volume (if applicable) and diluent (yellow boxes in Figure 1). Each profile will automatically calculate the volume of drug required based on the drug concentration (green box in Figure 1); as well as automatically calculating the volume of diluent for reconstitution of vials (not shown), final concentration of the infusion, and expiration (the latter are in purple in Figure 1). Before being placed on a shared electronic computer drive, every electronic IV profile card is triple checked by three pharmacists and is saved in a manner to not allow alterations. During actual utilization, each profile still requires an independent double check to make sure all required information is present.
Figure 1 Example of an electronic IV chemotherapy profile card. The information in the pink colored boxes is generated from the information in the yellow boxes.
An electronic IV profile for hazardous medication preparation eliminates errors that may result from a hand-written preparation profile card. These errors include handwriting legibility, human errors associated with transcription and calculation errors.
An electronic IV profile offers other benefits in patient safety and cost effectiveness. By utilizing a standard format for instructions, variability in wording and differences in compounding are eliminated; allowing one method and less chance of compounding errors. Pharmacist time can be spent providing other clinical services as it takes less time to fill out an electronic document versus manually reviewing guidelines and hand-writing compounding instructions.
One of the barriers we encountered when implementing electronic IV profile cards was the vast array of chemotherapy medications that are seen within the pediatric population. The library of electronic IV profile cards was started with the common chemotherapy medications seen in our institution. If a new medication is ordered, our old hand-written profiles are utilized until an electronic version can be constructed.
A survey was conducted of the eleven pediatric pharmacists who utilize the electronic IV profile cards. Strengths identified included: faster processing time, standardization amongst orders, increased safety as there is less chance for human or calculation errors, and ease of use. Possible weaknesses identified included: possible calculation errors (volume of medication or diluent) if electronic IV profile card is not double checked, IV guidelines of institution are less likely to be checked, in-stock product verification may not be done to ensure product listed on profile card is currently stocked, and difficulty with navigation if the computer is not compatible with the electronic profile program. Some respondents suggested expanding the drug library to include more chemotherapy agents and changing storage from the electronic computer drive to the pharmacy intranet to allow for more accessibility throughout the hospital. All respondents stated they were comfortable and satisfied using the electronic IV profile cards and preferred the electronic system to the handwritten paper format.
Overall the introduction of electronic IV profile cards has increased pediatric pharmacist satisfaction in preparing IV profile cards and improved the safety of the preparation of IV profile cards. In the future, we hope to expand the chemotherapy agents available in the electronic IV profile card library and look into alternative methods for storage of the electronic IV profile cards.
New Practitioners Network
Precepting: A PGY2 Pharmacy Resident’s Perspective
by Ryan Szynkarek, PharmD, PGY2 Resident at the University of Chicago Medical Center
As a nearly finished PGY2 Internal Medicine Pharmacy Resident, I am proud to say that I am the product of over 30 different preceptors’ teachings, with each preceptor implementing their own unique teaching style. I am writing this article to share how I have adopted these great teaching styles into my own precepting style, my observations as a novice preceptor, the challenges I have overcome, and my recommendations to any new preceptor.
My preceptors have exhibited a number of exceptional qualities and skills. First off, they are elite pharmacy role models. They are highly respected by their medical teams. They earned this respect through their professionalism and quality patient care, which is elevating the profession as a whole. Preceptors who possess passion for their practice area have in turn made me passionate for that area as well. When I precept, I make it a point to show the passion that I have, which I find engages my pharmacy students and residents. An additional and necessary quality for a preceptor is patience. Pharmacy trainees all present with a varying array of baseline knowledge and skills. If the preceptee does not understand a basic concept, the preceptor must invest the time needed to teach the trainee instead of getting frustrated. Preceptors must empower those being precepted. For pharmacy students, allowing them to make recommendations to the team allows them to realize that they are directly impacting patient care. For pharmacy residents, giving them the necessary tools and opportunities to make independent evidence based recommendations, even if it deviates slightly from what you would have done (given that it is safe and efficacious for the patient), will allow them to develop into independent practitioners. Feedback is required by all pharmacy schools through evaluations and for most pharmacy residencies via ResiTrak. As a preceptor in my own right, I try to emulate the best preceptors I had and make it a point to provide positive feedback along with the constructive feedback to help my trainees recognize things they are doing correctly and motivate them to continue to work hard and grow.
As a novice preceptor, I have made a few interesting observations and overcome a number of unique challenges. I realized that pharmacy students and residents first approached me with their questions instead of their more experienced primary preceptor. I believe that as a recent graduate, I may have been more approachable than the primary preceptor. In terms of challenges, my initial challenge was time-management. Balancing time between my clinical responsibilities and precepting my pharmacy student or resident was difficult. By having a daily plan (e.g. making a rotation calendar) one can better manage both the clinical and precepting responsibilities. Recognizing my own knowledge limitations was another unique challenge. Even though as a preceptor I wanted to answer all of their questions, I had to accept that I was learning myself and did not have all of the answers. Instead, these became great opportunities for us to learn together and for me to model how to find the answer to their question versus asking the preceptor. The last unique challenge was how to provide teaching points for a PGY1 pharmacy resident. I found it fairly easy to provide teaching points to pharmacy students. However, pharmacy residents have a larger knowledge base, making it difficult to provide teaching points while trying to learn the specialty-area myself. Following a discussion with my preceptor, I identified global teaching points to provide to the PGY1 resident such as working-up patients, presenting patients, and assisting with interventions.
Precepting is an esteemed way to give back to the profession of pharmacy, and the transition from student preceptor has been a rewarding one for me. I consider myself fortunate to have encountered so many quality preceptors and it is through my experiences with these preceptors that I have been able to personalize my own precepting style.
The GAS From Springfield
Are we there yet?
by Jim Owen and Scott Meyers
Yes, kids, we are there. The spring 2014 session of the 98th General Assembly has been adjourned. Your life, liberty and property are safe for the time being, but who knows how long that will last? Pharmacy dodged some big bullets for the time being during this session. There was a lot of pressure on Senator Tony Munoz to move the Biosimilar bill SB1934, but he resisted. He told us he would hold it, and he did. The proponents of this bill grow in number, and if the FDA doesn’t act this year, we could face a different situation in the Fall Veto Session or next spring.
We also dodged a license fee increase. We believe that is a result of a revised budget process relating to state grants to the public colleges of pharmacy in Illinois. We’re still not sure if the colleges are going to receive any money this year, but it does seem certain that it won’t come from the coffers that the Department of Financial and Professional Regulation oversee, if they receive any funds at all. This one may come back to haunt us in the fall, too, so you can bet we’re keeping our eyes and ears open and our bargaining chips close at hand.
Good news for the Illinois Poison Center! At least for four more years. A legislative maneuver with the Medicaid budget will provide $2Million in funding annually for the next four years. After that, it’s anyone’s guess as to where the money will come from. Part of the process involves federal matching funds and some assistance to a hospital in DuPage County. The Poison Center staff is already gearing up to build alliances and hopefully work more directly with the state’s many 911 centers to develop a better and more sustainable source of funding in the future. We are very supportive of that. We know, through the trials and tribulations of the state’s public colleges of pharmacy, what it’s like to never really know if there will be any funding next year, so we will watch and support them as they develop their next plan.
In the grander scheme of things, the budget that was passed was technically balanced if you assume the recommended transfers and borrowing can take place. The pension debt and its accompanying issues remain with little evidence that they will be addressed anytime soon. The General Assembly left the temporary income tax alone this session so unless something is done during the veto session, your state income tax will revert to 3.75% of your income on January 1, 2015. A lot will depend on who is elected Governor in November for this issue. Either way, it won’t be pretty.
We both encourage each of you to take some time this summer and connect with your State Representative and Senator. And if they are up for re-election (all of the Representatives are, by the way), then connect with their opponent if they have one. Learn how they stand on health care in general and pharmacy in particular. Offer to be a resource for them when the sessions begin again in November and January. Make a contribution to their campaign fund if you believe they are a friend to your profession. This is a great time of year for all of that with fund raisers, county fairs, festivals and parades. Don’t pass up a chance to say hello.
And don’t forget the ICHP Pharmacy Action Fund. The $1K Raffle is underway, and it’s a great way to support pharmacy. The Auction With A Twist returns this fall, too, and now is a great time to put together a team to sponsor a great auction prize. Grab a few co-workers, fraternity brothers, or even your golfing buddies and buy an iPad, Surface, flat screen or other great prizes to help us generate more contributions for the PAC. Go to the ICHP website at www.ichpnet.org and go to the Public Policy page for more information.
Finally, thank you for reading this column and keeping track of the important legislation and regulation that will impact us all. You are the grassroots of the ICHP advocacy effort. You can and do make a difference in your profession!
College Connections
Cultivating Communication
by Katherine Sencion, P2, University of Illinois at Chicago College of Pharmacy
As future pharmacists, communication is a necessary skill that we ought to continuously work on. We have all learned the theories in our classes: We have been taught the difference between verbal and nonverbal cues; we have come to understand the difference between closed and open-ended questions; for the most part, we know what to do when barriers to communication present themselves. Those theories are essential for our profession, but it is even more important to put them into practice. Some students have been lucky enough to have experiences in pharmacies that improve their communication skills. These students know what works and what does not work when interacting with patients, insurance companies, and coworkers. However, for the rest of us without such experiences, communication may not come as easily, and we must continue to improve.
While there are many settings in which such skills can be developed, my involvement with ICHP has been the most opportune setting for me. With the responsibility of organizing hospital tours for each of the four hospitals near the UIC College of Pharmacy campus, I became increasingly comfortable communicating and networking with various pharmacists and managers in the area. I learned the significance of e-mailing etiquette, which at first seemed trivial, until I became attentive to proper subject lines and the difference between Cc and Bcc. Nowadays, first impressions are made not in person, but rather through technology; well written e-mails are now as important as a well tailored suit.
I also improved my communication skills through my participation in Legislative Day, perhaps my favorite ICHP event. Legislative Day encourages students to step outside of their comfort zone and pushes them to communicate with various legislators and pharmacists from the state. My experience at Legislative Day was eye-opening – I learned that with effective communication, seemingly intimidating legislators and directors transformed into individuals with whom I could carry on a conversation. While students may at first feel overwhelmed with the activities of Legislative Day, they finish the night with confidence, having successfully communicated with legislators and networked with fellow pharmacists, lobbyists, and students.
This year, I will continue my involvement as our chapter’s President-Elect, a role that I am honored to be in and excited to begin. With my newfound confidence that has developed throughout my experience as the chapter’s P1 liaison, I hope to increase active involvement among our student members. Each year, we have various events that go beyond biweekly general body meetings, including lung health events, P4 roundtables, and multiple networking events. My first goal is to reach out to my classmates and heighten awareness of such opportunities. My second goal is to increase participation in and delineate particular activities for our chapter’s committees on lung health and mental health awareness. The activities that our committee members engage in have proven to have a positive impact on our community, and I hope to continue to strengthen our work. Following from our responsibility to our community, my last goal is to collaborate with other student organizations in order to have more interactions with patients and increase counseling opportunities.
It is evident that these goals will only continue to strengthen the communication between our chapter and its members, and I hope that this communication will carry over to our workplaces and continue to improve the profession of pharmacy.
Pura Vida
by HollyAnn Russell, P4, Professional Practice Chair, SIUE School of Pharmacy
 Pura Vida! This is something one would hear daily upon traveling to Costa Rica. It translates into, “the pure life.” Costa Rica is a beautiful country, no more than the size of Kentucky. It has the greatest biodiversity per square foot in the world. However, only a small percentage of the rainforest has been discovered and used for medicinal purposes. For these reasons, major conservation efforts are occurring to save the rainforest. Ten years ago, SIUE partnered with the National Park of Carrera, Costa Rica to support the exploration and protection of the rainforest and its species. I was fortunate enough to have the opportunity to travel to this exotic country for a ten-day study abroad trip. SIUE School of Pharmacy recently initiated a new independent study with a focus on medicinal plants and tropical disease states. The trip is a component of the course to aid students in their learning and to experience a different culture of pharmacy.
Pura Vida! This is something one would hear daily upon traveling to Costa Rica. It translates into, “the pure life.” Costa Rica is a beautiful country, no more than the size of Kentucky. It has the greatest biodiversity per square foot in the world. However, only a small percentage of the rainforest has been discovered and used for medicinal purposes. For these reasons, major conservation efforts are occurring to save the rainforest. Ten years ago, SIUE partnered with the National Park of Carrera, Costa Rica to support the exploration and protection of the rainforest and its species. I was fortunate enough to have the opportunity to travel to this exotic country for a ten-day study abroad trip. SIUE School of Pharmacy recently initiated a new independent study with a focus on medicinal plants and tropical disease states. The trip is a component of the course to aid students in their learning and to experience a different culture of pharmacy.
 The first few days of travel were spent in the nation’s capital, San Jose. Here we were welcomed into the University of Costa Rica School of Pharmacy. Pharmacy school in Costa Rica is far different than that in the U. S. The program is five years and six months long with a strong focus on industry. In fact, students have industrial courses where they are assigned rats to inject drugs into in order to study the effects of the drug as a realistic experience. After meeting with several faculty members at the school, we learned that they desire to model their school more after pharmacy schools in the U.S. They want to push pharmacists into a more clinical role and are exploring ways to adjust their curriculum. This makes it easy for U.S.-educated pharmacists to be accepted in Costa Rica.
The first few days of travel were spent in the nation’s capital, San Jose. Here we were welcomed into the University of Costa Rica School of Pharmacy. Pharmacy school in Costa Rica is far different than that in the U. S. The program is five years and six months long with a strong focus on industry. In fact, students have industrial courses where they are assigned rats to inject drugs into in order to study the effects of the drug as a realistic experience. After meeting with several faculty members at the school, we learned that they desire to model their school more after pharmacy schools in the U.S. They want to push pharmacists into a more clinical role and are exploring ways to adjust their curriculum. This makes it easy for U.S.-educated pharmacists to be accepted in Costa Rica.
 Costa Rica operates on universal health care. The country has public and private hospitals. The public hospitals are government funded. All citizens have a percentage of wages taken every month to support the system. They are then issued a card indicating they are a citizen contributing to the system. Everyone’s card looks the same; therefore everyone receives the same level of healthcare regardless of their financial standing. When sick, citizens go to a public hospital, show the card, and receive treatment at no cost. However, there are also private hospitals. These private institutions receive no government funding. Citizens have the option of going to either public or private hospitals. Why would citizens pay out of pocket if they are paying into the universal care? Private hospitals provide a higher level of care and less wait time for treatment but they lack certain specialties and equipment that may drive a citizen to the public hospital regardless. What about pharmacy?
Costa Rica operates on universal health care. The country has public and private hospitals. The public hospitals are government funded. All citizens have a percentage of wages taken every month to support the system. They are then issued a card indicating they are a citizen contributing to the system. Everyone’s card looks the same; therefore everyone receives the same level of healthcare regardless of their financial standing. When sick, citizens go to a public hospital, show the card, and receive treatment at no cost. However, there are also private hospitals. These private institutions receive no government funding. Citizens have the option of going to either public or private hospitals. Why would citizens pay out of pocket if they are paying into the universal care? Private hospitals provide a higher level of care and less wait time for treatment but they lack certain specialties and equipment that may drive a citizen to the public hospital regardless. What about pharmacy?
Pharmacy also has private and public domains. Public pharmacies operate in a similar fashion as the public hospitals. What we consider “chain pharmacies” in the US are considered “private pharmacies” in Costa Rica. The issue of the public pharmacies is the drugs themselves. The government often buys drugs in bulk in an attempt to obtain the lowest cost. Unfortunately, this may result in poorly formulated products, lack of bioequivalence, and incomplete formularies. Private chains are there to offer patients better options, consisting of name brand drugs and better formulated generics with an overall greater selection. The issue of the private chains is that patients pay out of pocket and there are little regulations. Besides a small list of restricted medications, patients can go to the pharmacy without a prescription and purchase medications at the pharmacist’s discretion. Pharmacists are well-respected professionials in Costa Rica. Most citizens will go to the pharmacy before they will go to the hospital. This demonstrates that pharmacists are one of the most trusted and easy to access healthcare professionals around the world!
This trip was an eye-opening and life-changing experience. Costa Rica is a beautiful and diverse country with the most welcoming individuals. Exposure to another culture of pharmacy is highly beneficial within one’s educational career. While there was a great deal of learning that took place, there was also a lot of exploring of the rainforests, wild life, beaches, and amazing food. Study abroad trips are increasing within the world of pharmacy. And I highly recommend one to Costa Rica. Pura Vida!
A Student Pharmacist’s Introduction to MTM
by Akorede Dada, P3, Chicago State University College of Pharmacy
The American Pharmacists Association (APhA) defines Medication Therapy Management (MTM) as services that seek to enhance care by improving collaboration between pharmacists, physicians and other health care providers; enhancing communication between patients and their health care team; and empowering patients to optimize medication use for improved health care outcomes.1 MTM has been discussed in my classes as an initiative incorporating pharmacists as the best qualified health care professionals to help patients effectively use their medications. Of the various Introductory Pharmacy Practice Experiences (IPPE’s) I completed, my Applied Practice Skills Community Practicum stands out because I was given the opportunity to provide MTM services within a retail pharmacy chain and understand firsthand the positive impact that these services produce.
My preceptor’s goal during this IPPE was to provide me with an environment to experience the typical day-to-day tasks of a pharmacist, as well as the new services they were providing. After performing medication history reviews, my preceptor presented the opportunity to perform an MTM interview. She explained the reimbursement protocol for the pharmacy, how the patients were selected, the options for completing MTM that included either in person interviews or phone calls, and how she effectively incorporated MTM responsibilities into the workflow.
Before performing MTM, I called potential patients to set up a day where they could either visit the pharmacy with all of their medications or have them readily available at home during a phone call. My first MTM session was a phone call, and lasted about 20 minutes. This patient was on over 7 medications, so reviewing the dosing, how the patient was actually taking the medication, adverse effects, and possible drug interactions provided me with the opportunity to apply everything I had learned thus far in school.
I initially asked if the patient was taking anything over-the-counter (OTC), and she said no. Later in the interview, I discovered she was taking aspirin, which she didn’t initially associate as being an OTC medication. From this I learned that it’s very important how questions are asked.
I inquired about the patient’s proton pump inhibitor (PPI), which was initiated after the most recent hospitalization and had no known indication. This led me to contact the patient’s primary care provider (PCP), and I discovered that the patient was on it for stress ulcer prophylaxis in the hospital, and ended up getting discharged on it. This intervention led to discontinuing the PPI and removing the unnecessary medication and additional expense. This demonstrates how MTM services can be beneficial during transitions of care, as a patient transitions from the inpatient to the outpatient setting. At the end of the session I recorded all of my findings electronically, created a pharmacy care plan that was given to the patient, and sent the claim in for reimbursement.
The entire experience was rewarding and insightful. It incorporated many skills and reinforced my commitment to the pharmacy profession. I was able to improve patient care by ensuring patients were taking medications appropriately and checking for any medication-related problems. I see how performing MTM can be valuable during transitions of care to prevent rehospitalizations. It is my aspiration that future pharmacy rotations will yield such positive and meaningful outcomes.
Reference:
More
Officers and Board of Directors
TOM WESTERKAMP Immediate Past President224-948-1528 tom_westerkamp@baxter.com
LINDA FRED
President-Elect
Welcome New Members!

| New Member |
Recruiter |
| Seema Patel |
|
| Lindsey Westerhof |
|
| Nadia Tancredi |
Helen Afolarin |
| Katherine Miller |
|
| Rachel Bentley |
Don Ferrill |
| Jordan Meyer |
Margaret Heger |
ICHP Pharmacy Action Fund (PAC) Contributors
Names below reflect donations between July 1, 2013 and July 1, 2014. Giving categories reflect each person's cumulative donations since inception.
ADVOCACY ALLIANCE - $2500-$10000
Edward Donnelly
Dave Hicks
Frank Kokaisl
Michael Novario
LINCOLN LEAGUE - $1000-$2499
Scott Bergman
Kevin ColganAndrew Donnelly
Ginger Ertel
William McEvoy
Scott Meyers
Michael Rajski
Carrie Sincak
Michael Weaver
Patricia Wegner
Thomas Westerkamp
CAPITOL CLUB - $500-$999
Rauf Dalal
Linda Fred
Ann Jankiewicz
Jan Keresztes
Kathy Komperda
Despina Kotis
Mary Lynn Moody
UIC Student Chapter
Jill Warszalek
GENERAL ASSEMBLY GUILD - $250-$499
Margaret Allen
Pete Antonopoulos
Michael Fotis
Janette Mark
Jennifer Phillips
Edward Rainville
Heidi Sunday
SPRINGFIELD SOCIETY - $100-$249
Jennifer Arnoldi
John Esterly
Travis Hunerdosse
Carrie Vogler
Marie Williams
Cindy Wuller
William Wuller
GRASSROOTS GANG - $50-$99
Susan Berg
Jennifer Ellison
Tory Gunderson
Robert Hoy
Mike Koronkowski
Evanna Shopoff
Jerry Storm
CONTRIBUTOR - $1-$49
John Chaney
Irvin Laubscher
Zakarri Vinson
Upcoming Events

Thursday, July 3
Champion Webinar: Women's Health
LIVE Webinar
Thursday, July 17 at 12:00pm & Tuesday, July 22 at 3:00pm
Champion Webinar: "Low T" and Testosterone Therapy: the Good, the Bad, and the Ugly
LIVE Webinar
Friday, August 1
Student Leadership Retreat
Roosevelt University College of Pharmacy | Chicago, IL
Monday, August 6
ICHP Central Region Family Night at the Ballpark
Springfield Sliders vs. Danville Dans
Robin Roberts Stadium at Lanphier Park | Springfield, IL
Wednesday, August 20
Deadline! Early Bird Deadline and Hotel Room Deadline for ICHP 2014 Annual Meeting
Thursday, September 11 - Saturday, September 13
ICHP 2014 Annual Meeting
Drury Lane | Oakbrook Terrace, IL
Tuesday, September 9 at 3:00pm & Wednesday, September 17 at 12:00pm
Champion Webinar: Women's Health
LIVE Webinar
Tuesday, November 4 at 3:00pm & Thursday, November 13 at 12:00pm
Champion Webinar: Dosing in Hepatic Failure
LIVE Webinar

Print Entire Issue