Print Entire Issue
March is Illinois Poison Prevention Month!

KeePosted Info
Features
March is Illinois Poison Prevention Month!
2014 Spring Meeting
NPN Night at the Ballpark
Calling NPN Volunteers
Meet Amanda Peerboom
Deadline Approaching
Columns
President's Message
Directly Speaking
Educational Affairs
Board of Pharmacy Update
Leadership Profile
The GAS From Springfield
New Practitioners Network
College Connections
A P3’s Viewpoint of Midyear
Advancement and Reflections
My Experience at the ICHP Annual Meeting Residency Showcase
The Role of PPMI in Pharmacy Education
More
Officers and Board of Directors
Welcome New Members!
ICHP Pharmacy Action Fund (PAC) Contributors
Upcoming Events
KeePosted Info
 Illinois Council of Health-System Pharmacists
Illinois Council of Health-System Pharmacists
4055 North Perryville Road
Loves Park, IL 61111-8653
Phone: (815) 227-9292
Fax: (815) 227-9294
www.ichpnet.org
KeePosted
Official Newsjournal of the Illinois Council of Health-System Pharmacists
EDITOR
Jacob Gettig
ASSISTANT EDITOR
Jennifer Phillips
MANAGING EDITOR
Scott Meyers
ASSISTANT MANAGING EDITOR
Trish Wegner
DESIGN EDITOR
Amanda Wolff
ICHP Staff
EXECUTIVE VICE PRESIDENT
Scott Meyers
VICE PRESIDENT - PROFESSIONAL SERVICES
Trish Wegner
DIRECTOR OF OPERATIONS
Maggie Allen
INFORMATION SYSTEMS MANAGER
Heidi Sunday
CUSTOMER SERVICE AND
PHARMACY TECH TOPICS™ SPECIALIST
Jo Ann Haley
ACCOUNTANT
Jan Mark
COMMUNICATIONS MANAGER
Amanda Wolff
LEGISLATIVE CONSULTANT
Jim Owen
ICHP Mission Statement
Advancing Excellence in the Practice of Pharmacy
ICHP Vision Statement
ICHP dedicates itself to achieving a vision of pharmacy practice where:
- Pharmacists are universally recognized as health care professionals and essential providers of health care services.
- Patients are aware of the training, skills, and abilities of a pharmacist and the fundamental role that pharmacists play in optimizing medication therapy.
- Formally educated, appropriately trained, and PTCB certified pharmacy technicians manage the medication distribution process with appropriate pharmacist oversight.
- Pharmacists improve patient care and medication safety through the development of effective public policies by interacting and collaborating with patients, other health care professionals and their respective professional societies, government agencies, employers and other concerned parties.
- Evidence-based practices are used to achieve safe and effective medication therapies.
- There are an adequate number of qualified pharmacy leaders within the pharmacy profession.
- Pharmacists take primary responsibility for educating pharmacy technicians, pharmacy students, pharmacist peers, other health professionals, and patients about appropriate medication use.
KeePosted Vision
As an integral publication of the Illinois Council of Health-System Pharmacists, the KeePosted newsjournal will reflect its mission and goals. In conjunction with those goals, KeePosted will provide timely information that meets the changing professional and personal needs of Illinois pharmacists and technicians, and maintain high publication standards.
KeePosted is an official publication of, and is copyrighted by, the Illinois Council of Health-System Pharmacists (ICHP). KeePosted is published 10 times a year. ICHP members received KeePosted as a member benefit. All articles published herein represent the opinions of the authors and do not reflect the policy of the ICHP or the authors’ institutions unless specified. Advertising inquiries can be directed to ICHP office at the address listed above. Image disclaimer: The image used in the Pharmacy Tech Topics™ advertisement is the property of © 2014 Thinkstock, a division of Getty Images.
Copyright © 2014, Illinois Council of Health-System Pharmacists. All rights reserved.
Features
March is Illinois Poison Prevention Month!
Pharmacists can play a big role in preventing harm!
by Scott A. Meyers, Executive Vice President
Every year over 80,000 calls are made to the U.S. Poison Centers. Illinois is fortunate to have one of them based in Chicago. In addition, Illinois hospitals treat thousands of accidental poisonings each year.
What are you and your colleagues doing to help prevent accidental poisonings? Do you hang poison prevention posters in the halls of your hospital? Do you provide poison prevention presentations to grade school classes, PTO groups or other interested organizations? How about setting out informational table tents with poisoning statistics and facts on the tables in the cafeteria during this important observance?
If you haven’t thought about it, you’ve got plenty of time to plan. If you’re already planning your activities, add taking photos to your list of things to do. We would love to hear and share what you do for Poison Prevention Month and National Poison Prevention Week (March 16-22). (Please obtain signed permission from those photographed if faces are visible in order to be displayed in KeePosted. Without signed releases we will have to blur or disguise the folks in the pictures.)
Poison Prevention is just one of the many roles a pharmacist can play and your active involvement in that role can and should be highlighted. If you need ideas for activities to highlight Poison Prevention Week or Month, go to the Illinois Poison Center’s website at http://illinoispoisoncenter.org/ or the National Poison Prevention Week website at http://www.poisonprevention.org/poison.htm where you will find a variety of activities and products. You can make a difference for your community and play a big role in preventing harm!
2014 Spring Meeting
March 28-29, 2014 | Bloomington-Normal, IL
Spring into action and take bold steps for patient care by attending the 2014 ICHP Spring Meeting. The primary focus of the educational programming is on quality initiatives to improve patient care and healthcare outcomes.
Sandra A. Van Trease, BBA, Executive MBA, will be the keynote speaker discussing Accountable Care Organizations (ACOs). An ACO is defined by the Centers for Medicare and Medicaid Services as “an organization of health care providers that agrees to be accountable for the quality, cost and overall care of Medicare beneficiaries who are enrolled in the traditional fee-for-service program who are assigned to it.” What does this mean for pharmacists and pharmacy technicians? How does this impact Pharmacy Services and patient outcomes? Those questions will be answered by our keynote, who is group president for BJC HealthCare in St. Louis, MO (please refer to her full bio on page 4 of the web brochure).
Continuing in the focus on quality outcomes and patient care, the Spring Meeting educational programming will include pharmacist involvement in transitions of care, adverse event reporting and identification, quality measures, review of new therapeutic guidelines, pharmacy best practices and how to incorporate students in quality initiatives and research.
Let’s make bold strides for our patients by learning how to implement quality initiatives in Illinois institutions through educational programming, the poster session and exhibit program! Enjoy some social time while supporting pharmacy legislative issues at the ICHP PAC event* Friday night of the meeting.
*separate fee required to attend
Register Now and take advantage of Early Bird pricing! (until March 4, 2014)
Make sure to reserve your hotel room by March 4, 2014!
Educational Programming and Meeting Highlights:
- Earn up to 9 CPE Hours!
- Keynote Speaker Sandra A. Van Trease on ACOs
- Transitions of Care Pharmacy
- Quality Measures
- Student Involvement in Pharmacy Practice
- Break-Out Sessions:
- Pharmacy practice
- Clinical pharmacy
- Other activities:
- Exhibit program
- Poster session
- Town hall meeting
- ICHP PAC Fund Poker Party (separate fee required to attend)

Make sure to download
ICHP's Spring Meeting Mobile App for the most up-to-date Spring Meeting content - now available in app stores!
NPN Night at the Ballpark
Chicago Cubs vs Chicago White Sox
Tuesday, May 6, 2014
7:05 pm
Tickets are $24
Upper deck reserved seats, section 508.
All ICHP new practitioners, pharmacy residents, residency directors, and preceptors are welcome. Only ICHP members may attend and only one ticket per person may be purchased. Your credit card will be charged when you order.
Ticket sales are open through Friday, April 25 (or until they're gone) -- after that date, all remaining tickets may be sold to an outside party.
Calling NPN Volunteers
Calling all students and recent graduates ( < 10 years), join the New Practitioners Network for our 2nd Annual networking and volunteer event at the Lurie Ronald McDonald House (211 East Grand Avenue, Chicago, IL) on Sunday, April 13th, 2014 from 10am-Noon. We will be preparing brunch to serve to the 70+ people staying at the house and want your help*!
Register online here. Registration deadline is March 1st.
Volunteers will be responsible for bringing and/or preparing food at the event, meal set-up and clean-up. Additionally, volunteers are invited to join the guests for the meal that we prepare. A sign-up sheet of food items will be sent out closer to the date of the event.
*Due to a limited amount of space, we will be accepting the first 20 volunteers (Space will be limited to 2 students per school.)
If you wish to help with the event but cannot attend, we will be accepting monetary donations to help cover the cost of food. Please contact Jan Mark at 815-227-9292.
Meet Amanda Peerboom
How I Got Where I Am Today
 I grew up in the Rockford area, went to Christian Life High School, and then went to Rock Valley College for my pre-pharmacy course work. I am a fourth year pharmacy student currently on an elective rotation with ICHP and will be graduating this May from Chicago State University.
I grew up in the Rockford area, went to Christian Life High School, and then went to Rock Valley College for my pre-pharmacy course work. I am a fourth year pharmacy student currently on an elective rotation with ICHP and will be graduating this May from Chicago State University.
During my first year at Rock Valley College (RVC), I was not sure what I wanted to do, so I focused on getting some general education courses completed. Later that year I began to feel desperate to try to figure out what I wanted to choose as my career choice. I had taken a few online personality quizzes that suggest different career choices based on your answers, and I always seemed to get caught up with the ones listed at the top. The lists were always in alphabetical order, so I found myself picking things like accountant, architect, and actuary. Finally my boyfriend (now husband) took me to the student center and had me use their assessment tool for deciding careers and majors. He suggested I start in the middle of the list, which ended up being several pages long. I eventually came across pharmacist, and for some reason that one stood out to me.
I decided I would do some research about the job duties and requirements. I liked how it seemed to be a little more challenging than some of the other options. I am the first in my family to go to college, so I was determined to pick something that would make them proud. I began imagining how I would be able to help friends and family with the drug and health knowledge I would learn. The thought of all the helpful knowledge I would obtain through pharmacy school was enough to encourage me to aim for this high goal, so I decided to pursue pharmacy as a career. I found out what classes were needed and began creating my plan on how to get into pharmacy school.
One summer at RVC, my aunt convinced me it would be a good idea to take the Pharmacy Technician class the school offered. I agreed with this since I really had little idea what pharmacy was like and everything that pharmacists did. After taking the class, I became a certified technician and was looking for a way to get some experience in a pharmacy. I approached my teacher and got the opportunity to volunteer at the hospital where she worked, Swedish American Hospital. I spent every Friday volunteering there during my last semester at RVC. That following summer I was given the opportunity to work there during my summer and winter breaks as a student worker, along with a few other students. I loved the time I spent working there and would always look forward to coming back each break. Working at this hospital helped inspire me further to become a pharmacist.
 The application process to get into pharmacy school is very lengthy. I can’t even recall how much time I actually spent on everything required for the PharmCAS application and some of the supplemental items different schools require. I’m glad I was able to stay motivated and didn’t miss anything on the application website. It was an extremely exciting day when I received a phone call from Chicago State University, offering me the opportunity to be in their program.
The application process to get into pharmacy school is very lengthy. I can’t even recall how much time I actually spent on everything required for the PharmCAS application and some of the supplemental items different schools require. I’m glad I was able to stay motivated and didn’t miss anything on the application website. It was an extremely exciting day when I received a phone call from Chicago State University, offering me the opportunity to be in their program.
Pharmacy school has been very tough at times, but now that I am on rotations it seems to be more enjoyable. I can’t believe how much I have learned over the past few years. Initially I was very nervous about rotations, because I didn’t feel like I was ready. That is the amazing part of rotations; it helps you apply what you have been studying the previous years in the classroom. You build more confidence, and things begin to click in your mind by making more sense than they did when you were just studying the material in the classroom.
During my rotation here with ICHP, I hope to learn a lot more about this organization. I have been a member during all four years of pharmacy school. I went to the meetings that were held at school, Legislative Day, and I have also been to one of their Spring Meetings, which was the first professional meeting I had attended. I enjoyed going to that meeting; there were interesting topics and some topics were specific to students. I have also written a couple of articles for KeePosted. I know this organization has a focus on pharmacy legislation. To be honest, law was not one of my strengths in school, and I hope my rotation at ICHP will help strengthen my knowledge and confidence of pharmacy law.
There are some other fun things that have kept me busy for the past year along with pharmacy school. I just recently got married to my high school sweetheart. We also recently bought a house that we have been fixing up. Originally the plan was to wait until after I graduated, but we couldn’t wait any longer. I still can’t believe we decided to do all of this during my last year of pharmacy school, but everything has been working out well so far. I am looking forward to graduation, passing the licensing exams and finally practicing as a pharmacist!
Deadline Approaching
Pharmacists and Techs Need to Be Relicensed by March 31
Reminder:
Columns
 President's Message
President's Message
Decisive
by Mike Fotis, ICHP President
What does decisive mean to you? Based on the title, you might assume this book is all about making quick decisions, but the purpose of Decisive is to describe “How to make better choices in life and work”.1 Decisive provides a lot of worthwhile advice, and Chip and Dan Heath do not spend a lot of time offering platitudes to solve real life problems. The platitude type of book offers nothing new and is usually a waste of time. You know…like a book with an entire chapter about the importance of good communication, which makes me think, “Oh you are saying good communication is important? No wonder I can’t get ahead. I thought bad communication was the way to solve problems!” You might have noticed this is one of my pet peeves!
Decisive served as the basis for discussion at the ICHP Leadership Retreat this past November.
Some of the most useful suggestions are summarized below. I think this information can help to set up a framework to identify better personal and professional choices.
- Search for alternative points of view
In clinical practice, one of the first things I check when selecting a review article for guidance is to see if the authors searched for alternative points of view and considered opposing findings in their search methods. After all, how useful would a clinical review be if the authors only considered articles that agreed with their point of view? We should remember to apply this method to decision making. We all need to protect our thinking from confirmation bias, and seeking opposite points of view is a good way to get a sense of how sound our thought process is. No need to follow the example set by politicians who seem to never be able to consider a different point of view. Rather, it is important to search just as hard for evidence that contradicts your point of view as it is for evidence that tends to support a point of view.
A good research paper describes their results by including 95% confidence intervals. We can adopt this thinking to non-clinical decision making. Many assumptions go into decision making. Taking a moment to consider your own confidence in each assumption can go a long way towards preventing poor decisions and act as a break against overconfidence. Don’t forget The Beatles were rejected by one recording label thinking that a 4 piece group was passé as everyone “knew” that popular music was moving exclusively to solo singers like Elvis. The Chicago Cubs decided against keeping Greg Maddux as everyone “knew” only power pitchers were capable of compiling a winning record.
It is so easy to fall into the trap of narrow framing. We do this every time we decide based on a whether or not statement. If there are only two choices to decide from, most likely the decision is based upon narrow framing. Of course we can have too many choices and end up with paralysis by analysis. However, whenever we are faced with binary options, it’s time to think about a third and possibly a fourth choice before making a decision. Thinking outside of the box is all about considering more than the stated options. For example: Should you keep your job, or should you leave and do a PGY1 residency? If you like the job you have right now maybe a third option is to approach your boss about setting up a non-traditional residency? Not possible? Perhaps your boss would be willing to help you to gain residency equivalent experiences? Why you might even present your project at an ICHP meeting! I am not suggesting one of these is THE RIGHT ANSWER for you, but instead I’m suggesting that you avoid only binary choices and consider one or two additional alternatives. Another way to avoid narrow framing is to consider “vanishing options”. What would you do if you COULDN’T choose one of the binary choices?
- Consider opportunity costs
Opportunity costs include time as well as money. What else could you do with your savings if you didn’t purchase an expensive investment? What else could you accomplish if an unnecessary workload function was identified and eliminated? Tech-Check-Tech comes to mind as an example. A second example: Many pharmacy departments are assigning entry-level departmental responsibilities to experiential students instead of to pharmacists. In addition to reducing opportunity costs, pharmacists are performing other duties while the students take over, and these departments have avoided the binary choice, “Should we have our pharmacists do this duty or not?”
- Consider the risk and cost of inaction
Some problems require a bold decision. Success may be difficult to achieve. Before deciding to delay or even to table an idea, spend a few minutes considering the impact of a likely outcome if we fail to act. Often we forget that taking no action is still a decision.
- Gain distance to minimize emotions
Decisions affect family members, colleagues, and patients. A lot of emotions come into play. The authors offer a number of suggestions to help to gain distance. Think of these suggestions as a method to gain distance. These suggestions are not implying that you ignore concerns of family, colleagues, etc.
- Professional decisions: What would you decide if you were brand new to the organization?
- Personal decisions: If a close friend was facing the same choices, what would you advise?
- All types: Use a 10-10-10 strategy. What would you think about the problem in 10 minutes, 10 days and in 10 years?
What else would have to be true for choice A to be the best option? For Choice B and Choice C? What is your confidence in these assumptions? One technique I used often at the P&T Committee was to ask an overzealous advocate for a new drug, “If this new drug is so good, why can’t we take the old drug off the formulary?”
- Honor your core priorities
What kind of person (parent, spouse, coworker, teacher, clinician) do you want to be? What is your purpose? Please don’t allow a “B” priority to interfere with “A” level priorities. The authors used an example faced by volunteer agencies. Their question (note the narrow framing): “On mission trips should volunteer clinicians be allowed to bring along their families during surgery?” Your decision is “yes” if satisfying the volunteers is your purpose, but the answer is “no” if safe surgery is your purpose. We should also change the whether or not statement to include other options for family.
Of course as a leader you can’t make everyone happy. BUT you can conduct a decision making process that insures that everyone is heard, that core priorities are recognized, and that important and creative options are considered. Using a process that all parties recognize as fair builds your strength as a leader. How a leader makes decisions goes a long way toward building a successful team.
Reference:
Heath C, Heath D. Decisive: How to Make Better Choices in Life and Work. New York: Crown Business; 2013.
 Directly Speaking
Directly Speaking
Did You Get Lost In December?
by Scott A. Meyers, Executive Vice President
While this article appears in the February KeePosted, I’m writing it less than 10 days after December 2013! So hopefully you won’t think to yourself “It’s February, why’s he talking about December?” when you read this. But I know I got lost in December this year and after just signing a large stack of member non-renewals, I’m hoping many more of our members did the same.
Let me tell you how I got lost. It wasn’t really lost in the conventional “I don’t know where I am” sense, and it wasn’t even lost in space. It was lost in time. I spent the first 5 days of December in Florida on vacation with my lovely wife and two good friends, Mike and Jackie Novario. We hit Universal Studios, Disney World and Epcot, and the west coast – specifically Anna Maria Island and Sarasota. It was fun, it was warm, and it was action packed! Then I followed that up with 5 more days in Orlando for the ASHP Midyear Meeting. Always a great opportunity to see old friends, make new ones and learn a lot.
By the time I got home, winter had more than taken over with -8° temps, a solid blanket of white and plenty of traffic accidents and road salt for everyone. The holidays were immediately upon me and because of the late date of Midyear, it seemed like the gift shopping pressures were magnified. Can I get an Amen?!
To compound issues, I had not managed my annual allotment of vacation well and had 10 days left to use or lose in the already shortened month. I know, my fault, quit whining. But when you’ve been out of the office for a week already and then try to take another two work weeks off in the last three, something had to give. I didn’t get all ten burned, but that’s ok because come January 1st, the bank gets refilled, and who wants to take time off in the first 2-3 months of the calendar year unless a trip to the tropics is on the table?
Christmas got here so quickly, I missed a lot of the build-up of anticipation and didn’t even feel the December 26th “It’s over already” let down. I spent a significant amount of time during my days off monitoring and responding to work emails and visited the office to sign papers or checks. But most of you pharmacy directors and clinical specialists deal with this too when you don’t leave town for vacation, so I really don’t expect or want sympathy.
By New Year’s Eve, December was a blur. There were lots of great memories but also a lot more distractions this past year than I think I’ve ever noticed. Again, the weather didn’t help! New Year’s Eve for Lana and I was dinner at Steak and Shake and an early showing of “The Hunger Games: Catching Fire”. We were safely in the house in spite of the 8 inches of snow long before the ball dropped in Times Square!
So now into the first full week of January, I’m starting to catch up! I’m dealing with issues that I could have taken care of in December if there weren’t so much of everything else to do. I’m guessing many of you are in the same boat. It does help that a new module for APPEs for most of Illinois’ Colleges of Pharmacy started this week because it helped me get back in my groove a little quicker than I might usually do. ICHP has a student on rotation during the first module of 2014, Amanda Peerboom from Chicago State University. I’m sure most of your sites have new students too which hopefully helps you get back into full swing more quickly after the holidays. Although I’ve heard from a few friends and members that it doesn’t seem to slow down anymore during the holidays or ever!
So I’m asking you, did you get lost in December this year? Did time sneak past you more rapidly than usual? Was it the Midyear or the Holidays or merely family that caused it for you? Next year the Midyear is late again, as is Thanksgiving. I think Thanksgiving was another big contributor for me! So while I’m sure we’ll all forget this article fairly quickly, maybe it would be valuable to go to your Outlook, or whatever day planner/calendar you regularly use, and put some reminders in October and early November this year to remember that December is going to zoom by just like this last year’s did. Add a note to hang your outdoor Christmas decorations a week or two before Thanksgiving but promise not to turn them on until Black Friday. October 1st is my birthday, so when you’re all out shopping for my gift in late September, add to that reminder to start looking for specials on potential Christmas and Hanukkah gifts for your loved ones! And most importantly, if you’re like me, make sure you take more days off this spring, summer and fall when the weather is beautiful, rather than realizing when it’s almost too late that you’ve got too many days left in the bank.
I hope your New Year has started out well and is rapidly rolling along toward a beautiful spring! And plan ahead as I hope to, so that you don’t get lost in December this year!
Educational Affairs
Optimizing Premedications to Prevent Antineoplastic Related Infusion Reactions
by Brenton Bialik, 2014 UIC College of Pharmacy PharmD Candidate and Jonathan Kinscherff, PharmD, Clinical Oncology Pharmacist, Swedish American Regional Cancer Center, Rockford, IL
 Infusion reactions (IRs) due to chemotherapy and monoclonal antibodies (MoAbs) are well documented and preventing them is crucial to maintaining patient safety. The majority of systemic antineoplastic agents are associated with the possibility of eliciting a reaction. The agents most commonly associated with IRs are the taxanes, platinum compounds, epipodophyllotoxins, asparaginases, and MoAbs.1,2 With many new chemotherapy drugs in the pipeline, it is imperative for pharmacists to develop their understanding of how to prevent IRs. This article will focus on the etiology of IRs, pharmacologic and non-pharmacologic pretreatment strategies, and current research developments that pharmacists can use to optimize patient care.
Infusion reactions (IRs) due to chemotherapy and monoclonal antibodies (MoAbs) are well documented and preventing them is crucial to maintaining patient safety. The majority of systemic antineoplastic agents are associated with the possibility of eliciting a reaction. The agents most commonly associated with IRs are the taxanes, platinum compounds, epipodophyllotoxins, asparaginases, and MoAbs.1,2 With many new chemotherapy drugs in the pipeline, it is imperative for pharmacists to develop their understanding of how to prevent IRs. This article will focus on the etiology of IRs, pharmacologic and non-pharmacologic pretreatment strategies, and current research developments that pharmacists can use to optimize patient care.
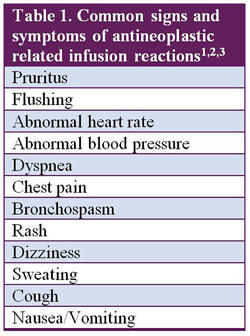 Infusion reactions, regardless of etiology, present with a similar set of signs and symptoms (Table 1). The most common IRs are type I hypersensitivities caused by immunoglobulin E (IgE) mediated release of histamine, leukotrienes, and prostaglandins.3 Phase 2 and 3 studies revealed that 41% of patients who received paclitaxel for ovarian or breast cancer experienced hypersensitivity reactions.4 Although many studies refer to these reactions as hypersensitivity reactions, not all reactions are true allergic reactions mediated by IgE. These reactions present similarly, but are believed to result from direct effects on immune cells by antineoplastic agents themselves or by their metabolites.5 Thus, the term infusion reaction will be used throughout this article.3
Infusion reactions, regardless of etiology, present with a similar set of signs and symptoms (Table 1). The most common IRs are type I hypersensitivities caused by immunoglobulin E (IgE) mediated release of histamine, leukotrienes, and prostaglandins.3 Phase 2 and 3 studies revealed that 41% of patients who received paclitaxel for ovarian or breast cancer experienced hypersensitivity reactions.4 Although many studies refer to these reactions as hypersensitivity reactions, not all reactions are true allergic reactions mediated by IgE. These reactions present similarly, but are believed to result from direct effects on immune cells by antineoplastic agents themselves or by their metabolites.5 Thus, the term infusion reaction will be used throughout this article.3
The prevalence of IRs can be highly variable, so prevention is key. IRs may occur immediately during the first infusion or may take several treatments to manifest. MoAbs tend to elicit IRs during the initial infusion.3 With chemotherapy, the risk largely depends on the agent used. Carboplatin IRs, for example, increase after repeated exposures, typically peaking after the 6th infusion.1 Being familiar with the typical onset of a reaction can help optimize pretreatment strategies.
Pharmacists play a key role in optimizing a patient’s pretreatment therapy. Both non-pharmacologic and pharmacologic pretreatment options are used to prevent or reduce the severity of IRs.1,5 Non-pharmacologic options (Table 2) begin by obtaining thorough histories from patients prior to treatment.3 A history of multidrug reactions and prior reaction to drugs of the same chemical class are indicators that the patient may be more likely to develop reactions. Next, optimizing the route and rate of the infusion as well as modifying the order in which medications are administered may reduce the likelihood of a reaction.3 Lastly, skin testing may help to identify the likeliness of an IR but has limited utility in practice.5 Identifying patients who are more likely to develop reactions allow practitioners to be vigilant with both pretreatment regimens and precautionary measures.
 Pharmacologic options for prophylaxis typically include histamine H1 and H2 receptor antagonists (RAs) plus corticosteroids.1 Acetaminophen may also be used prior to MoAb administration.3 Appropriate pretreatment can reduce the rate of serious IRs by over 50%.5 However, not all chemotherapy regimens that have a high IR incidence benefit from the use of premedication, such as platinum compounds and epipodophyllotoxins.5 Test doses may be useful for certain agents but may not always correlate with onset and severity of IRs. Test doses are commonly performed before administering bleomycin, although a review of bleomycin test dose literature found that fatal IRs can occur with any dose.6 Therefore, test doses for bleomycin are not predictive of IRs. Regardless of the approach, it is essential to utilize both non-pharmacologic and pharmacologic options to ensure patient safety.
Pharmacologic options for prophylaxis typically include histamine H1 and H2 receptor antagonists (RAs) plus corticosteroids.1 Acetaminophen may also be used prior to MoAb administration.3 Appropriate pretreatment can reduce the rate of serious IRs by over 50%.5 However, not all chemotherapy regimens that have a high IR incidence benefit from the use of premedication, such as platinum compounds and epipodophyllotoxins.5 Test doses may be useful for certain agents but may not always correlate with onset and severity of IRs. Test doses are commonly performed before administering bleomycin, although a review of bleomycin test dose literature found that fatal IRs can occur with any dose.6 Therefore, test doses for bleomycin are not predictive of IRs. Regardless of the approach, it is essential to utilize both non-pharmacologic and pharmacologic options to ensure patient safety.
Patients with additional comorbidities may benefit from a tailored approach of pretreatment regimens. Research for optimization of pretreatment regimens is ongoing. For example, the current standard pretreatment for preventing paclitaxel-related IRs is oral dexamethasone administered 12 and 16 hours prior, and H1 and H2 RAs given intravenously (IV) 30 minutes before the infusion.7 Berger and colleagues recently discontinued all premedications in 55 breast cancer patients who did not experience IRs after the first two doses of paclitaxel.8 Subsequent doses resulted in zero IRs, which suggests that after 2 doses of paclitaxel, discontinuing premedications may be considered in some patients. Braverman and colleagues tapered dexamethasone in 115 patients receiving biweekly paclitaxel who did not experience IRs after the first dose.9 Zero patients experienced IRs during the taper including 46 patients who eventually discontinued dexamethasone and continued paclitaxel treatment.
Further research on the subject is warranted, but these findings convey promise for patients who experience adverse reactions to premedications. In the case of paclitaxel, diabetic patients who experience blood glucose fluctuations due to corticosteroids may be able to discontinue pretreatment in future cycles. Reducing or eliminating unnecessary drug exposure in patients under-going taxing chemotherapy regimens may also improve quality of life.
Patients receiving cancer treatment are already under an increased amount of stress. After obtaining accurate and complete patient histories, pharmacists can and should ensure patients are properly premedicated to help prevent IRs. Proper premedication may entail adding an agent or removing an agent. Ongoing research will allow for continued optimization of premedication regimens with the goal of preventing IRs while maintaining patient quality of life.
Take-home points
- Infusion reactions can be caused by nearly all antineoplastic agents, but taxanes, platinum compounds, epipodophyllotoxins, asparaginases, and monoclonal antibodies are most commonly associated with infusion reactions.1,2
- Both non-pharmacologic and pharmacologic measures are utilized to prevent or reduce the severity of infusion reactions.
- Research on premedication regimens is ongoing. Further optimization of regimens will result in fewer infusion reactions and fewer adverse events related to premedication.
References:
- Zanotti KM, Markman M. Prevention and management of antineoplastic-induced hyper-sensitivity reactions. Drug Saf. 2001;24(10):767-79.
- Lenz HJ. Management and preparedness for infusion and hypersensitivity reactions. Oncologist. 2007;12(5):601-9.
- Vogel WH. Infusion reactions: diagnosis, assessment, and management. Clin J Oncol Nurs. 2010;14(2):E10-21.
- Paclitaxel package insert. New York, NY: Pfizer Labs; 2011 Dec.
- Lee C, Gianos M, Klaustermeyer WB. Diagnosis and management of hypersensitivity re-actions related to common cancer chemotherapy agents. Ann Allergy Asthma Immunol. 2009;102(3):179-87.
- Lam MS. The need for routine bleomycin test dosing in the 21st century. Ann Pharmacother. 2005;39(11):1897-902.
- Bookman MA, Kloth DD, Kover PE et al. Intravenous prophylaxis for paclitaxel-related hypersensitivity reactions. Semin Oncol. 1997;24(6 Suppl 19):S19-13-S19-15.
- Berger MJ, Dunlea LJ, Rettig AE et al. Feasibility of stopping paclitaxel premedication after two doses in patients not experiencing a previous infusion hypersensitivity reaction. Support Care Cancer. 2012;20(9):1991-7.
- Braverman AS, Rao S, Salvatti ME et al. Tapering and discontinuation of glucocorticoid prophylaxis during prolonged weekly to biweekly paclitaxel administration. Chemotherapy. 2005;51(2-3):116-9.
- Raisch DW, Campbell W, Garg V et al. Description of anaphylactic reactions to paclitaxel and docetaxel reported to the FDA, with a focus on the role of premedication. Expert Opin Drug Saf. 2011;10(4):521-8.
- Jevtana package insert. Bridgewater, NJ: sanofi-aventis U.S. LLC; 2013 May.
- Shepherd GM. Hypersensitivity reactions to chemotherapeutic drugs. Clin Rev Allergy Immunol. 2003;24(3):253-62.
- Dillman RO, Hendrix CS. Unique aspects of supportive care using monoclonal antibodies in cancer treatment. Support Cancer Ther. 2003;1(1):38-48.
- Rituxan package insert. South San Francisco, CA: Genentech, Inc; 2013 Aug.
- Erbitux package insert. Branchburg, NJ: ImClone LLC; 2013 Aug.
- Torisel package insert. Philadelphia, PA: Wyeth Pharmaceuticals Inc; 2012 June.
- Doxil package insert. Horsham, PA: Janssen Products; 2013 Aug.
Board of Pharmacy Update
Highlights from the January Meeting
by Scott A. Meyers, Executive Vice President
The January 14th Board of Pharmacy Meeting was held at the James R. Thompson Center in downtown Chicago. These are the highlights of that meeting.
New Board of Pharmacy Member – Dr. Prem Rupani introduced himself as the newest public member of the Board of Pharmacy. Dr. Rupani is a board certified internal medicine specialist on staff at Mt. Sinai, Holy Cross and Little Company of Mary hospitals in Chicago. He is currently President of the medical staff at Holy Cross.
Pharmacy Practice Act Rules Update – General Counsel for the Department and the Governor’s staff are currently reviewing the final draft of rules and once they have completed that process, they are expected to be published in the Illinois Register which opens up a 45-day public comment period. Once the comment period ends the comments will be evaluated and revisions may be made. The revised draft is then submitted to the Joint Committee on Administrative Rules for final approval. There is no confirmed publication date, but the Rules are hopefully going to be approved sometime this spring or summer.
Legislative Update – Garth Reynolds, IPhA Executive Director provided the Board with a brief update on current legislation before the General Assembly. In addition to bills from last session, which may appear again in this session, two other noteworthy bills were mentioned. HB3671 introduced by Rep. Mary Flowers, D-Chicago, would remove the prior authorization requirements for drugs prescribed in excess of the 4 drug limit that currently exists for public aid patients. SB2585 introduced by Sen. Dan Kotowski, D-Park Ridge, would standardize all third party payer prior authorization rules including allowing pharmacists to initiate the process and requiring a response to prior authorization requests within 48 hours or the prescription is automatically approved.
There will be more bills introduced over the next few weeks, so the Board will rely on the associations (ICHP and IPhA) to keep them informed.
Visitor Comments – For the last several meetings, the Board has opened the floor for visitor comments on pharmacy related topics and the discussion during this time was on one specific topic. Medical marijuana, while not yet available in Illinois, is now legal and the rules are being finalized. Joe Friedman, licensed Illinois pharmacist, informed the Board that he personally intends to apply for a medical marijuana dispensatory license when they are available. He additionally urged the Board of Pharmacy to get involved in the rule making because even though the current law does not specifically call for pharmacists to dispense the product (and federal law would prohibit pharmacies from dispensing) because who knows medications better than pharmacists? Jim Smeeding, Executive Director of the National Association of Specialty Pharmacies, also spoke to the Board and urged involvement of pharmacists and the Board. The Association believes that it is the pharmacist’s role to educate the patients and the public with regard to medical marijuana and its proper use. Finally James O’Donnell, an assistant professor of pharmacology at Rush Medical College and former editor of ICHP’s KeePosted, urged the Board to get involved in the rule making process, too. O’Donnell stated that studies have found marijuana to be safer than alcohol and that pharmacists are the drug experts who should be in control of its use. He recommended that the Board work with the Department and the General Assembly to make marijuana a schedule IV or V in Illinois because of its safety.
The board members were very engaged with the discussion and while no formal action was taken, their interest in the issue became much stronger as a result of the presentations by the visitors. (It should be noted that attendance at this meeting exceeded previous board meeting records significantly, at least in the last 22 years that I have been in attendance, with a large number of students, chain pharmacy representatives, and other interested parties. It is clear interest in these meetings continues to grow. The robust discussion during the meeting’s open discussion topic was not on the agenda, so it had no influence on the attendance of most of those present, the addition of the visitors’ comments portion to the current meetings may be responsible for drawing the larger audience.)
Next Board of Pharmacy Meeting – Is scheduled for Tuesday, March 11th at 10:30 AM on the 9th floor of the James R. Thompson Center in downtown Chicago. Pharmacists, pharmacy students and pharmacy technicians are welcome to attend the open portion of the meeting.
Leadership Profile
Kathryn Schultz, PharmD, BCPS
 Where did you go to pharmacy school?
Where did you go to pharmacy school? Midwestern University Chicago College of Pharmacy
Trace your professional history since graduation: where have you trained / worked, any special accomplishments? (include a description of your current area of practice and practice setting)
Before pharmacy school I received a bachelor of science in cellular and molecular biology and then worked in a benchtop research lab at UIC investigating the molecular markers present for successful implantation of an embryo (successful pregnancy) and endometriosis. I realized that lab wasn’t for me and I needed to get out and talk to humans instead of my cell cultures!
I was able to gain some experience between graduation (Sept 2006) and starting residency by working at Good Samaritan Hospital and Epi-Q, Inc. I started my PGY1 residency at Rush University Medical Center in July 2007, then completed my PGY2 in Oncology at University of Michigan Hospital and Health System 2008-2009. In August 2009, I started as a Clinical Specialist in Hematology/Oncology/Cell Therapy at Rush University Medical Center.
Describe your current area of practice and practice setting.
My current practice setting is inpatient hematology/oncology/stem cell transplant. Although I have been temporarily off service to build Beacon (the Epic CPOE module for chemotherapy).
What initially motivated you to get involved, and what benefits do you see in being active in a professional association such as ICHP?
I joined ICHP as a student and became involved then. One thing that sparked my active involvement was frustration with the government in Illinois when it came to health care, so I attended Legislative Day starting as a student and then joined Government Affairs Division as a PGY1 and have been on the Division ever since. Politicians know politics, we know health care, so it is up to us to inform them how the laws and practice act actually impact health care in Illinois.
What advice would you give to a new practitioner eager to become more involved within ICHP? to the new grad? to the student?
Just join! Start with a local society meeting, such as NISHP, and start talking to people. NETWORK! Then find some smaller way to get involved—be a student liaison, join a task force, sit in on a local society meeting (they are open to all—you don’t have to have a current position on the board), ask a friend or colleague if you can join them for a Division such as Government Affairs, Professional Affairs, Educational Affairs, Marketing Affairs, etc.
Is there an individual you admire or look up to, or a mentor that has influenced your career?
There have been numerous individuals who have impacted my career. Starting with my cousin, Jim Dorociak, who discussed pharmacy career options when I was first considering pharmacy school, to ICHP’s most recent Pharmacist of the Year, Ann Jankiewicz—a colleague who manages her career, professional involvement and her family and reminds me that it can be done and done well.
As a newer practitioner, what is your vision for pharmacy in the future? Or what would you like to able to see accomplished within pharmacy?
I would like to see pharmacy getting a seat at the C-suite table and that this be an expectation at all hospitals so that pharmacy is always a part of planning for the future as part of an interdisciplinary team.
What three adjectives would people use to best describe you?
I asked a few pharmacist friends about this question and of the answers I received, here are the ones that can be printed:
Dedicated, persistent, energetic
Do you have any special interests or hobbies outside of pharmacy/work/school? special accomplishments?
I did my first triathalon a couple years ago and a couple of half-marathons the past year along with some 10K’s and 5K’s.
Do you have a favorite restaurant/food?
I love restaurant week in Chicago and go a little crazy each year planning out the new places I’m going to try.
What is your favorite place to vacation?
Lake Namekagon (remote place in the Northwoods of Wisconsin where cell phones don’t work!)
What is the most interesting/unique fact about yourself that few people know?
My bucket list includes touring all of the MLB baseball stadiums. I have 3 slated for this spring.
Anything else, you would like to share?
I have 2 Siberian huskies that were rescued from an animal shelter. Einstein is almost 16 years old and Snow is 9 years old.
The GAS From Springfield
“And They’re Off!”
by Jim Owen and Scott Meyers
If you’ve ever been to a horse race, you’ll recognize “And they’re off!” as the first thing you hear when the starting gates open during each race. Well, the starting gates have opened for the Illinois General Assembly for the Spring 2014 Legislative Session, but the irony is there’s little hurry in Springfield at this early stage of the race to Memorial Day. As a matter of fact, most who monitor the deliberations in Springfield would probably laugh if they heard that phrase used in conjunction with the beginning of the session.
Last year’s spring session gave us over 6200 bills to sift through, and this year will probably follow suit. Although this year is supposed to be a budget year (it seems every year is a budget year) which means other bills are kept to a minimum, our guess is that it will not have a serious impact on the numbers. A scary fact is that many of last year’s 6200+ bills are still alive in addition to the new ones that have been or will be introduced.
The new bill introduction deadline in the Senate is January 31st and February 14th in the House. Legislators who intend to move initiatives this session must at least have a vehicle introduced by those dates. But a vehicle can be something as basic as an addition and deletion of the same word in the existing Act that is expected to be changed. This can include the Pharmacy Practice Act, the Controlled Substance Act, the Hospital Licensing Act, the Hypodermic Needle and Syringe Act or several other acts that impact pharmacy and health care. So even though there are deadlines, they are only artificial. If you’re at all interested in seeing how many vehicle bills or technical changes are introduced at the beginning of the session, just go to www.ilga.gov/legislation/default.asp and open up any group of 100 bills in the Senate or the House and see how many have a title that ends with TECH. The good news is that very few if any will have something to do with pharmacy techs.
The next deadline requires House or Senate Substantive Bills to be passed out of Committee by March 28th in both chambers. This deadline is a little more helpful as there are often many vehicle bills that are introduced that are never intended to be used. In addition, many substantive bills that are introduced have little or no chance of making it out of committee because they lack merit, have an unpopular sponsor or are too controversial to ever move. Once this deadline has passed we should know what will be moving and what won’t. But one of our goals is to stop the bad bills before they even make it out of their first committee.
So what do we expect to see this year? The Biosimilars bill will surely rear its silly head again, with some biologic manufacturers attempting to create rules at the State level before the FDA actually allows them to be considered biosimilar or interchangeable. Talk about wasting everyone’s time and energy! There will probably be some new restrictions on hydrocodone containing products, too. While the federal government has not made a final decision, the continued growing abuse of hydrocodone containing products will probably cause our legislature to take some intermediary steps. Not making these products Schedule II’s but rather limiting the amounts that may be dispensed at any time. We will probably see some more tweaks to the Public Aid Code. The four prescription prior authorization requirement is under fire, and who knows what will actually be done.
There is no doubt this session will have its challenging issues, and there is also no doubt we will do our best to keep our patients safe and the profession moving forward. But for now, we can truly say, “And they’re off!”
New Practitioners Network
The Schweitzer Fellowship: A Mentee’s Perspective on Mentorship
by Bernice Man, P3, SSHP President, Chicago State University College of Pharmacy
 I have regularly visited Chicago’s Chinatown neighborhood with family and friends since moving to Chicagoland in the early 1990s. My reasons for coming to Chinatown have expanded from eating the delicious food to improving the health literacy of older adults who live there. I am currently serving as one of thirty-two 2013-2014 Chicago Area Schweitzer fellows. The Albert Schweitzer Fellowship is a service fellowship with a goal to cultivate future healthcare leaders who will address health disparities and improve health outcomes for underserved communities. The 2013-2014 Chicago Area Schweitzer fellows include students from medicine, nursing, optometry, social work, public health, art therapy, dentistry, psychology, law, and disability studies. Each fellow is required to create and complete a yearlong, 200-hour service project that addresses a health need in an underserved community under the guidance of multiple mentors.
I have regularly visited Chicago’s Chinatown neighborhood with family and friends since moving to Chicagoland in the early 1990s. My reasons for coming to Chinatown have expanded from eating the delicious food to improving the health literacy of older adults who live there. I am currently serving as one of thirty-two 2013-2014 Chicago Area Schweitzer fellows. The Albert Schweitzer Fellowship is a service fellowship with a goal to cultivate future healthcare leaders who will address health disparities and improve health outcomes for underserved communities. The 2013-2014 Chicago Area Schweitzer fellows include students from medicine, nursing, optometry, social work, public health, art therapy, dentistry, psychology, law, and disability studies. Each fellow is required to create and complete a yearlong, 200-hour service project that addresses a health need in an underserved community under the guidance of multiple mentors.
My Schweitzer project takes place in Chinese American Service League (CASL) Senior Housing, which is a government subsidized, residential housing complex near Chinatown Square. The project’s goal is to improve the health literacy of Chinese older adults by providing disease state presentations, medication reviews, and health screenings. The site population’s main barrier to healthcare is language. The vast majority of the residents speak various dialects of Chinese and have very limited English proficiency. For this reason, I have presented all materials in Cantonese, and have included topics such as arthritis, cholesterol, blood pressure, eye disorders, and cold/flu symptoms.
The Schweitzer Fellowship requires that each fellow have four different mentors, including an academic mentor, student mentor, advisory council mentor, and site mentor, who all serve to provide guidance on various aspects of the fellow’s project. My site mentor is Virginia Lai, the social service coordinator at CASL Senior Housing. Because she is the person most familiar with my site’s population, Ms. Lai has provided great insight into what health topics would be of most interest and of most use for the CASL Senior Housing residents. She has also helped me to foster a bridge of trust between the residents and myself by introducing me to the residents and promoting my project’s services. The academic mentor is an educator at the fellow’s academic institution. My academic mentor is Dr. Diana Isaacs, one of my professors at Chicago State University College of Pharmacy and the Chair of the ICHP New Practitioners Network. She has provided vital guidance on the health education and pharmacy practice aspects of my project, as she reviews all of the disease state information and medication reviews before I present the material at my project site. The student mentor is a current healthcare student who served as a Chicago Area Schweitzer Fellow in previous years. My student mentor is Jordan Becerril, a third-year medical student at Rush Medical College. Because he recently completed the Schweitzer Fellowship, Jordan has been very helpful in providing feedback on different aspects of my project. The advisory council mentor is a healthcare professional who serves as a resource for the fellows. My advisory council mentor is Dr. Mark Stoltenberg, a former Chicago Area Schweitzer Fellow who is a current second-year resident physician at Northwestern University McGaw Medical Center. He has been helpful in my project’s development, as he has suggested further ways in which I can expand my project. Ray Wang, the Chicago Area Schweitzer Fellows Program Director, and Bonnie Ewald, the Chicago Area Schweitzer Fellows Project Coordinator, have both served as informal mentors for my project. They both have provided valuable suggestions on how I can improve my project and have helped me access various healthcare resources.
The mentorship provided to me has been invaluable, as I truly believe that I could not have made my project a success without my mentors’ advice and support. When I applied for the fellowship, I had theoretical ideas on what I wanted to do for my service project and hypothetical ideas on how I wanted to complete it. Putting my project ideas into practice would have been much more difficult and time-consuming had I not had mentors who had previous experience in different facets of my project and who were willing and able to guide me through my project’s development. I have grown because of my mentors’ experiences and their willingness to share the knowledge that they possess.
Because of the Schweitzer Fellowship experience and because of my mentors, I have become confident that I can tackle any project going forward and that I will find a way to make that project successful. Because of the relationships that I have developed with my mentors during the fellowship, I anticipate that my mentors will continue to be resources that I will contact in the future when I need counsel. During the past year, I have learned how important it is to have mentors who can help guide me not only in how to tackle a project, but also in how to direct my career path both during and after pharmacy school. Because of the great experiences that I have had with my mentors, the CSU-COP SSHP chapter started a P1 – P3 mentoring program where P3 students can give advice to P1 students about school. ASHP currently offers the Mentor Match program, where any ASHP member can be matched with a mentor or mentee based upon their preferences and profile. I encourage everyone to find mentors for themselves, and I hope to serve as a mentor for pharmacy students in the future.
College Connections
A P3’s Viewpoint of Midyear
by Emma Carroll, P3 at University of Illinois at Chicago, Chapter President
Who says that finals of P3 fall semester cannot be broken up by sitting poolside in Orlando, Florida and attending ASHP’s Midyear Clinical Meeting? Not only was I worried about attending Midyear because it was during finals week, I was also nervous about being a Midyear “newbie” and not knowing what to expect of this magical meeting I have heard so much about. For the past two and a half years I have heard about the madness of the Residency Showcase and the Midyear meeting. It seemed like it would be an eternity before I actually experienced it for myself. But the time came to see what it was all about this past December. I was given the opportunity to present a poster at the Midyear Student Showcase, with classmates Alexandra Habanek and Nadiyah Chaudhary, on behalf of our ICHP student chapter. Our poster highlighted the Lung Health Initiative which is an integral component of our student chapter.
To put it simply, I had an amazing experience at Midyear! It was not as scary as I had imagined, nor was I trampled at the Residency Showcase as many people warned about. I particularly enjoyed the student portion of the meeting that culminated in a talk from Ron Culberson, which was motivational, humorous, and left me feeling good about the next few days to come. At the student forum I had the opportunity to share ideas with student chapter leaders from across the country and learn from what they have done with their state affiliates. There were many other opportunities in which P3s could participate such as a CV review and Residency 101 and 102 informational sessions.
After the Student Showcase poster presentation, I attended the UIC gathering at a nearby hotel where I was able to catch up with friends who have moved on to residencies, and faculty with whom I might not otherwise get to chat. The following day was the first day of the Residency Showcase. It was urged that non-P4 students only attend the last hour of the session, which gave us ample time to browse the residency programs that were featured that day and get an idea of the landscape for what is to come next year. Begrudgingly, on Monday, evening we had to leave balmy Florida and come home to the December weather and our Tuesday final.
I highly recommend attending the Midyear Clinical Meeting as a P3 if you are able to go. Although not essential, it gave me a grasp of what it will be like next year when I attend as a P4 and also made me realize that it is not quite as intimidating as I thought it would be. Having said that, I’m sure that as a P4 next year, I might not find the Residency Showcase quite so undemanding.
Advancement and Reflections
by Jennifer Aguado, P3, SSHP President, Rosalind Franklin University College of Pharmacy
Our growing chapter is making excellent progress in advancing student chapter activities and opportunities this year. As the student chapter President, I was given the opportunity to assist our chapter advisor, Dr. Frank Hughes, with the organization of the preliminary rounds of our very first clinical skills competition at Rosalind Franklin University of Medicine and Science College of Pharmacy. This is the first year that we have had students from our school in attendance at the 2013 ASHP Midyear Clinical Meeting. Aside from the abundance of student pearl sessions that we participated in, we also attended the student award ceremony where we were given the opportunity to showcase our poster on one of the highlighted events as part of the “Share and Reapply” session.
The inaugural class is now in the third year of the pharmacy curriculum, which allows for advancement in the clinical opportunities that are available to participate in. The clinical skills competition is the newest addition to the opportunities available to our students. It provides an opportunity for our students to practice applying the skills and knowledge acquired in class and through simulations to providing direct patient care in collaboration with physicians. Our local competition was held on October 16th, 2013 and was a success, with eight teams participating. The winners of the local competition were RaeAnn Hirschy and Jennifer Rispens.
The winners and a few other third year students from RFUMS attended the 2013 ASHP Midyear Clinical Meeting for the first time. Attending as a third year student allowed each of us to go through the experience early on, which prepares us for when we return next year as residency applicants. After several interviews with the students who represented RFUMS at the meeting, they summarized their experiences in the national competition and in attendance of the programming as being a unique, challenging, rewarding, and a valuable opportunity in fulfilling their ultimate goals of being a clinical pharmacist.
As I reflect on my own experiences, I would agree that attending the meeting was valuable and rewarding. I confirmed my decision to apply for a residency and inherited a wealth of information on the application process. I attended, very briefly, the residency showcase to observe and acquire a vision of what it would be like in the near future as a potential residency applicant. I had the opportunity to meet with a number of individuals - students and practicing professionals - which allowed me to extend my professional network. It was a pleasant experience showcasing our highlighted event at the “Share and Reapply” session at the student awards ceremony. I was amazed to see all of the interesting community service opportunities that the other student chapters organized.
While I have only highlighted two very successful events added to the history of our student chapter this year, we continue to have more opportunities available. Our student chapter has a number of philanthropy events planned for the upcoming months. I am looking forward to the learning experiences and opportunities that will come from assisting with the organization and participation of those events.
My Experience at the ICHP Annual Meeting Residency Showcase
by Ruchi Patel, P3, SSHP/ICHP Member, Chicago State University College of Pharmacy
In addition to my studies at Chicago State University College of Pharmacy, I have enjoyed opportunities to participate in student organization activities. I am an active member in a number of student organizations, including SSHP. SSHP is one of the organizations on campus that helps student pharmacists grow in ways that enable them to be successful leaders and practitioners in health-system pharmacy. One of the events that I attended this past year was the 2013 ICHP Annual Meeting in Oakbrook Terrace, IL. It was the first professional meeting that I attended and I must say that the experience was truly beneficial.
I wanted to attend the ICHP Annual Meeting in order to gain insights about residencies in general so I can be more prepared when I attend the Residency Showcase at the ASHP Midyear Clinical Meeting next year. Because I am a third year pharmacy student, I found it very beneficial to walk through the residency showcase and get an idea about how it works. During this time, I was able to speak to a number of pharmacy residency directors and was able to gather information regarding their residency programs. I also had the opportunity to speak with current residents at a number of the residency booths. Speaking with the residents about their experiences gave me insight about the expectations for particular residency programs. The residents also talked to me about challenges that they go through during their residencies. For example, one of the PGY1 residents gave me great advice about time management. She told me that time management was initially an issue for her and that in order to avoid procrastinating, she needed to plan ahead of time and use various scheduling tools. A PGY2 resident’s suggestion to me was to prioritize tasks and set up due dates in order to stay on top of everything. Another resident suggested that I stay up to date on my clinical knowledge by reviewing different disease states, knowing drug therapy, analyzing clinical studies, and participating in journal clubs. She said that doing these activities would help improve my critical thinking skills. When it comes to making decisions about patient specific drug therapy, critical thinking skills will be most beneficial. One of the pharmacy residency directors explained that their program is greatly interested in candidates who have community volunteer experiences and leadership roles.
Because I went to the ICHP Annual Meeting Residency Showcase, I learned a lot of important information about residency programs that I had not considered before. From my interactions with the residency directors and residents, I concluded that much more is needed to get a residency aside from good grades. You need to have other experiences such as community volunteering, leadership roles, and research experience in order to separate yourself from other applicants. Time management and critical thinking skills are also essential. I will be able to utilize this knowledge when I apply for residency and when I attend the Residency Showcase as a fourth-year pharmacy student.
The Role of PPMI in Pharmacy Education
by Zak Vinson, P3, SIUE School of Pharmacy
Pharmacy has always been an evolving profession, and that fact is more prevalent now than ever. The Pharmacy Practice Model Initiative (PPMI) is currently changing the way other professionals view pharmacists and how pharmacists view their own role in health care. Many health systems are already implementing several PPMI goals, including “Tech-Check-Tech” programs, requiring proper training and credentials for pharmacists and technicians, and promoting more pharmacist-patient interaction. These are all tremendous steps in the right direction towards pharmacists being recognized as fully-capable health care providers nationwide.
In order to truly make PPMI a universal goal, starting from the root of the pharmacy profession is vastly important. Current pharmacy students will be relied upon heavily in the near future to understand and implement the goals of PPMI into their individual practice settings. In order for students to be able to have a firm grasp on this role, they need to be educated properly on each individual goal. Recently, the Southern Illinois University Edwardsville School of Pharmacy Student Society of Health-System Pharmacy (SIUE SSHP) worked with the Advanced Pharmacy Practice Experiential (APPE) faculty to compose a new way to prepare students for rotations and their future jobs. This student and faculty group worked to create a program that would allow students to learn the goals of PPMI and be able to evaluate how well practice sites were meeting those goals. In the third professional year of pharmacy school, students take a required APPE preparatory course that includes lecture and discussion about PPMI. Included in this discussion is a PPMI handout that was created by the previous ASHP liaison of the SIUE SSHP which summarizes the 5 goals of PPMI and the 26 individual measures. The APPE faculty also created a required competency for fourth professional year students to complete during hospital rotations. This competency consists of the students identifying how PPMI is being addressed and participating in PPMI activities at their hospital sites. This hands-on way of learning will not only help students become familiar with the new pharmacy model, but will also help preceptors learn from students to better exemplify the goals of the model.
While this educational model to teach about PPMI is important, it is not the only way to spread the word. Guest speakers from Illinois and the rest of the United States are willing to visit schools and share their views on applying PPMI to different practice settings. Proper education and advanced training for technicians is also vital to the betterment of pharmacy practice. While pharmacy schools do not train technicians, it is possible to invite technicians to the schools to listen to these guest speakers and potentially provide information on how additional training can be obtained. One of the goals of PPMI is for pharmacists to have appropriate training for the activities they perform in their scope of practice, thus supporting students who want to obtain a residency and board certification is essential. In order for students to be properly prepared for the evolving world that they will soon enter, schools of pharmacy and respective student societies must work together to create an atmosphere that exudes the goals of the Pharmacy Practice Model Initiative.
More
Officers and Board of Directors
TOM WESTERKAMP Immediate Past President224-948-1528 tom_westerkamp@baxter.com
LINDA FRED
President-Elect
217-383-3253 linda.fred@carle.com
GINGER ERTEL Treasurer 660-342-5022 gertel@msn.com CAROL HEUNISCH Secretary 847-933-6811 cheunisch@northshore.orgTRAVIS HUNERDOSSE Director, Educational Affairs thunerdo@nmh.org
JENNIFER ELLISON Director, Marketing AffairsJennifer.C.Ellison@osfhealthcare.org
DESI KOTIS Director, Professional Affairs
FRANK KOKAISL
Director, Government Affairs
JENNIFER PHILLIPS Assistant Editor, KeePosted 630-515-7167 jphillips@midwestern.edu KATHRYN SCHULTZ Regional Director North
JULIE BUCEK Student Chapter LiaisonUniversity of IL C.O.P. bucek@uic.eduNADIYAH CHAUDHARY President, Rockford Student Chapter University of IL C.O.P. nadi925@gmail.comJANEY YU President, Student ChapterMidwestern University C.O.P. janey.yu@mwumail.midwestern.edu
BERNICE MAN President, Student Chapter Chicago State University C.O.P. bman@csu.edu TRAMAINE HARDIMON Student Representative Chicago State University C.O.P thardimo@csu.edu ZAK VINSON President, Student Chapter Southern Illinois University Edwardsville S.O.Pzvinson@siue.edu
ALEX MERSCH President, Student Chapter Roosevelt University C.O.P. amersch@mail.roosevelt.edu
JENNIFER AGUADO President, Student Chapter Rosalind Franklin University C.O.P. jennifer.aguado@my.rfums.org SCOTT MEYERS Executive Vice President, ICHP Office 815-227-9292 scottm@ichpnet.org
ICHP AFFILIATES
PETE ANTONOPOULOS President, Northern IL Society (NISHP) JULIA SCHIMMELPFENNIG President, Metro East Society (MESHP) jschimmelpfen@sebh.org MEGAN METZKE President, Sangamiss Society memiller8@yahoo.com
ED RAINVILLE President, West Central Society (WSHP) 309-655-7331x ed.c.rainville@osfhealthcare.org
Vacant Roles at Affiliates —
President, Rock Valley Society; Southern IL Society; Sugar Creek Society
Welcome New Members!

New Member Recruiter
Cynthia Dorr-Harthan Angelia Dreher
Lisa McLaughlin
Daniel Mickleborough
Lisa Sowinski-Raff
Naeil Elhaj Andrew Donnelly
Steven McKenna
Teresa Lewis
Hailey Anderson Jennifer Austin
Christopher Reyes
Stacy Schmittling Brandi Strader
Kunal Desai Rebecca Castner
Charmaine Shafer
Joel Reddish Alicia Juska
Traiana Mangum
Nicole Banks
David Troupe
Kathy Wierzbicki
Mindee Phan
Hemangini Shah
Mia Schmiedeskamp
Lauren Pestka
Karen Kolodziej
Mihir Patel
David Keys Tobi Sondag
Jennifer Tryon
Joe Revak
Jim Home
ICHP Pharmacy Action Fund (PAC) Contributors
Names below reflect donations between February 1, 2013 and February 1, 2014. Giving categories reflect each person's cumulative donations since inception.
GENERAL ASSEMBLY GUILD - $1000 & More Scott BergmanKevin ColganEdward DonnellyGinger ErtelDave HicksFrank KokaislWilliam McEvoy
Scott Meyers
Michael Novario
Michael Weaver
Patricia Wegner
Thomas Westerkamp
SPRINGFIELD SOCIETY - $500-$999 Stephanie CrawfordRauf Dalal
CAPITOL CLUB - $250-$499
Margaret Allen
Vern Johnson
Janette Mark
Edward Rainville
Heidi Sunday
Jill Warszalek
LINCOLN LEAGUE - $100-$249
Anonymous
Marie Williams
GRASSROOTS GANG - $50-$99
Susan Berg
Jennifer Ellison
Tory Gunderson
Glenna Hargreaves
Jerry Storm
CONTRIBUTOR - $1-$49 John Chaney
Izabela Wozniak
Upcoming Events

Tuesday, February 11
CPE Event! NISHP Program: 8th Annual Leg Day 101: Preparing to be a Pharmacy Advocate
UIC College of Pharmacy | Chicago, IL
Tuesday, February 11
CPE Event! Sangamiss Program: Blood Cholesterol Management Guidelines: What changes should be made to pharmacy practice and why?
American Harvest Eatery | Springfield, IL
Wednesday, March 5
Pharmacy Legislative Day
State Capitol | Springfield, IL
Friday, March 28 - Saturday, March 29
2014 ICHP Spring Meeting: Taking Bold Steps for Patient Care
Marriott Hotel & Conference Center | Bloomington-Normal, IL
Sunday, April 13
NPN Volunteer Opportunity: Lurie Ronald McDonald House
Chicago, IL
Tuesday, May 6
NPN Cubs Game
Wrigley Field | Chicago, IL
_web578x100.png)
Print Entire Issue



.jpg)