Print Entire Issue

KeePosted Info
Columns
President's Message
Directly Speaking
Medication Safety Pearl
Board of Pharmacy Update
New Practitioners Network
The GAS From Springfield
ICHPeople
College Connections
Keys to Successfully Completing Research: A Student’s Perspective on the Mentor/Mentee Relationship
Keep Your Eyes and Ears Open
Professional Practice Makes Perfect
More
Officers and Board of Directors
Welcome New Members!
ICHP Pharmacy Action Fund (PAC) Contributors
Upcoming Events
KeePosted Info
 Illinois Council of Health-System Pharmacists
Illinois Council of Health-System Pharmacists
4055 North Perryville Road
Loves Park, IL 61111-8653
Phone: (815) 227-9292
Fax: (815) 227-9294
www.ichpnet.org
KeePosted
Official Newsjournal of the Illinois Council of Health-System Pharmacists
EDITOR
Jacob Gettig
ASSISTANT EDITOR
Jennifer Phillips
MANAGING EDITOR
Scott Meyers
ASSISTANT MANAGING EDITOR
Trish Wegner
DESIGN EDITOR
Amanda Wolff
ICHP Staff
EXECUTIVE VICE PRESIDENT
Scott Meyers
VICE PRESIDENT - PROFESSIONAL SERVICES
Trish Wegner
DIRECTOR OF OPERATIONS
Maggie Allen
INFORMATION SYSTEMS MANAGER
Heidi Sunday
CUSTOMER SERVICE AND
PHARMACY TECH TOPICS™ SPECIALIST
Jo Ann Haley
ACCOUNTANT
Jan Mark
COMMUNICATIONS MANAGER
Amanda Wolff
LEGISLATIVE CONSULTANT
Jim Owen
ICHP Mission Statement
Advancing Excellence in the Practice of Pharmacy
ICHP Vision Statement
ICHP dedicates itself to achieving a vision of pharmacy practice where:
- Pharmacists are universally recognized as health care professionals and essential providers of health care services.
- Patients are aware of the training, skills, and abilities of a pharmacist and the fundamental role that pharmacists play in optimizing medication therapy.
- Formally educated, appropriately trained, and PTCB certified pharmacy technicians manage the medication distribution process with appropriate pharmacist oversight.
- Pharmacists improve patient care and medication safety through the development of effective public policies by interacting and collaborating with patients, other health care professionals and their respective professional societies, government agencies, employers and other concerned parties.
- Evidence-based practices are used to achieve safe and effective medication therapies.
- There are an adequate number of qualified pharmacy leaders within the pharmacy profession.
- Pharmacists take primary responsibility for educating pharmacy technicians, pharmacy students, pharmacist peers, other health professionals, and patients about appropriate medication use.
KeePosted Vision
As an integral publication of the Illinois Council of Health-System Pharmacists, the KeePosted newsjournal will reflect its mission and goals. In conjunction with those goals, KeePosted will provide timely information that meets the changing professional and personal needs of Illinois pharmacists and technicians, and maintain high publication standards.
KeePosted is an official publication of, and is copyrighted by, the Illinois Council of Health-System Pharmacists (ICHP). KeePosted is published 10 times a year. ICHP members received KeePosted as a member benefit. All articles published herein represent the opinions of the authors and do not reflect the policy of the ICHP or the authors’ institutions unless specified. Advertising inquiries can be directed to ICHP office at the address listed above. Image disclaimer: The image used in the Pharmacy Tech Topics advertisement is the property of © 2013 Thinkstock, a division of Getty Images.
Copyright © 2013, Illinois Council of Health-System Pharmacists. All rights reserved.
Columns
 President's Message
President's Message
Is it Time to Get Involved?
by Mike Fotis, ICHP President
Why YOU should be a part of a Professional Organization
Of course if you are reading this article in KeePosted than you already recognize the importance of professional organizations. My hope is that perhaps one or two of the ideas presented in this column might be of interest to your students, colleagues and co-workers who might not be members of a professional organization. I hope you think so, and that you are also willing to share this article with them. Second, I promise not to try to guilt anyone into joining. Here are my 5 ideas:
All the other health professions are doing it
That’s right – our colleagues in Medicine and Nursing, Physician Assistants, Therapists, Hospitals, Hospital Executives, you name it – they all have professional organizations. Now I don't really think other organizations are actively trying to undermine our profession, but for example, a professional organization of physicians is bound to be working to promote the interests of their own physician members. Health-system pharmacists also play an important role in promoting and protecting the health of our fellow citizens. It is just as important for pharmacists to make sure that our concerns about medication safety, product integrity, and proper use of medications are heard by the leaders of Illinois as it is for any other medical profession. ICHP is our voice. It just makes sense for pharmacists to have the same opportunity to address our concerns as everyone else.
Associate with energetic and enthusiastic colleagues
I can’t think of a better way to renew my commitment to our profession than by associating with the many energetic, enthusiastic, and highly professional colleagues that are members of ICHP. Let’s face it – the practice of pharmacy can get to be a grind sometimes. Work is busy and stressful. Our patients are seriously ill. There are drug shortages, staff shortages, computer glitches and restrictive rules and regulations that can drive anyone to pack up their attitude and start mailing it in. But we also know that the defining characteristic of professionals is that we NEVER mail it in. The 35th patient of the day you see in clinic deserves the same attention as the first patient. We all know the 35th patient is a father, mother, son, daughter, husband, or wife of someone. Working with the outstanding professionals who are members of ICHP and knowing you are not the only one faced with this dilemma is a perfect way to keep your professional candle lit and shining brightly.
Find a mentor
Learn how to think instead of what to think – Learn how and when to ask questions instead of only how to answer questions – Learn to ask the necessary questions. Associate with other professionals who offer support when you need support and a push when you need to be pushed. When you’re ready, take your turn to serve as a mentor. Working with a mentor and serving as a mentor have been some of the most rewarding activities of my career.
Get out of your bubble and test your ideas with other professionals
All of us can end up in our workplace bubble. After all, “This is the way we do things at our hospital pharmacy.” These ideas have stood the test of time and trouble. They were put together by talented and hardworking colleagues. They work, they are useful, and they prevent mistakes. But our methods and procedures are not the only way to do things, and a very few of them might not be the best way to do things. One sure method to stay on the cutting edge is to test your ideas and procedures outside of your workplace. When you discuss these ideas with other talented and dedicated pharmacists who are not part of your day to day routine, you learn to be articulate, and of course to not take things for granted. Honing our craft outside of our workplace bubble is an excellent way to take one’s practice of pharmacy to a new and higher level and maybe to help others. Why not give it a chance?
Get out there and volunteer
Volunteering for an assignment can make your work life easier. That’s correct…I said easier! Volunteer for a project with an ICHP division. Choose an assignment that you know you are eventually going to complete at your workplace. Your results will benefit from the input of other experts, and chances are your actions will be more complete and cover every base all thanks to the support of other expert volunteers at ICHP. Why you might even save time by volunteering while coming across as the genius you really are with your workplace colleagues!
In every way I am such a fortunate man. In ICHP I have had the opportunity to serve 3 terms as a Division Director, one term as President-Elect and have just begun a term as President. There is one common thread I have observed as new members join the Board of Directors and as other Directors finish their terms. ICHP has a brief swearing in ceremony for new directors. You can tell from the looks on their faces they feel the same way I did when I was first sworn in. “What did I just get myself into???” I have also noticed the look on the faces of Directors as their term is concluded. I already know I am going to feel the same way. It is clear that a) every single director is sorry their term is over and b) they are so pleased that they took a chance and decided to volunteer. The time will come when it feels right for you to volunteer and to become an even more active member of ICHP. When it does, won’t you please join us?
 Directly Speaking
Directly Speaking
Give Your Technicians A Holiday Gift That Keeps on Giving!
by Scott A. Meyers, Executive Vice President
In National Lampoon’s Christmas Vacation, Clark Griswold (Chevy Chase) receives a membership to the Jelly of the Month Club as his Christmas Bonus and Cousin Eddie (Randy Quaid) overwhelmed and almost choking on his eggnog, expounds, “Clark, that’s the gift that keeps on giving throughout the entire year!” Every time I see a gift that has lasting value, I think of that scene and how it was not the case for Clark.
But if you’re a pharmacy director, a pharmacist that works with an outstanding certified technician, or a certified pharmacy technician that works with other outstanding certified technicians, you can give one or many of those techs a holiday present of ICHP membership that will keep on giving throughout the entire year. ICHP technician membership now includes free online access to ICHP’s home-study product Pharmacy Tech Topics™! That one benefit is a $45 value for the membership fee of $35!
And ICHP membership offers so much more. But first let’s focus on the value of Pharmacy Tech Topics™. PTT as I will refer to it from now on, offers 10 hours of continuing pharmacy education (CPE) annually, specifically designed for certified pharmacy technicians in four quarterly modules. Each module has one specific topic of focus, and the first module of each year, available on January 1 will provide either 2.5 hours of law or medication safety CPE. With a two year subscription or membership in ICHP, certified pharmacy technicians will be able to obtain all the CPE credits they need to recertify with PTCB. All modules provide ACPE credit and will be reported directly to CPE Monitor. That’s an important fact for the future as PTCB moves to use CPE Monitor to facilitate the recertification process. It’s coming soon.
The module topics are timely and useful. Module titles from 2012-2014 include:
Risk Evaluation and Mitigation Strategies
Updates on Psychoses and Schizophrenia
Updates in Hepatitis C Virus Treatment
New Drugs 2012
Ethics and HIPAA for Pharmacy Technicians
Cough, Sneeze and Sniffle: Management of Respiratory Infections
Mechanisms of Drug Interactions
Managing Multiple Sclerosis and Its Symptoms
Addiction and Recovery 101
Anticoagulants and Applicable Disease States for Pharmacy Technicians
Skin Cancer Prevention and Treatment
The Skinny on Obesity
You can see these modules cover a wide range of topics and all with the pharmacy technician in mind. The modules are published in January, April, July and October and are good for CPE credit for two years. So there’s plenty of time to take advantage of each module when you’re ready and when you need the credit.
The modules require the completion of a post-test with a passing score of 70% or better. The questions are multiple choice and are scored immediately. Once the technician passes the test, the statement of credit is available for printing or storage, and it is forwarded to CPE Monitor. No more file folders that can get lost, no more statements of credit that can disappear equally as easy.
Now wait, there’s more to this exciting offer! (You’ll hear that a lot this season!) ICHP membership also includes 10 issues of ICHP’s News Journal KeePosted. Published online, this news journal provides updates on legislation, regulation and educational offerings. It highlights what’s happening at the various colleges of pharmacy along with patient safety articles and more. In addition to the KP as we like to call it, your technician member will receive discounts on registration fees to both statewide educational meetings. CE offered during the Champion Webinars, offered bi-monthly (we’ll talk about the Champion’s Program in a later issue if you are not familiar with it) is also free with 0.5 contact hours of ACPE credit offered.
As you can see, there’s more than just PTT and additional options for obtaining the much desired CPE credit. And unfortunately, the days of the pharmaceutical industry sponsored supper-clubs that many of us grew up with and loved are long gone. With them the once abundant CPE programs for both pharmacy techs and pharmacists have gone, too. So ICHP has put together this new and improved technician membership package to make up for that. We know how hard it is to find good pharmacy technician CPE and how expensive it can be too.
So this holiday season, consider giving “a gift that keeps on giving throughout the entire year” to one or more of your Certified Pharmacy Technicians. And if you’re a Certified Pharmacy Technician and dropping hints doesn’t seem to be working, you can always treat yourself to this great value as your own holiday gift! Happy Holidays! And only 24 more shopping days till Christmas!
Medication Safety Pearl
An Analysis of Medication Errors Associated with Technology
by Jen Phillips, PharmD, BCPS (1,2) and Bonnie Bachenheimer, PharmD (2)
(1)Midwestern University Chicago College of Pharmacy, (2)Advocate Lutheran General Hospital
In the last 10-15 years, there have been a number of advancements in the area of automation and technology in the healthcare industry including, but not limited to: computerized prescriber order entry (CPOE), automated medication dispensing machines, smart infusion pumps, automated inventory management systems, barcode medication administration devices and medication compounding and preparation devices. Many of these advancements offer safety advantages compared to the manual systems they have replaced. As a result, many healthcare institutions have implemented some of these new technologies in an effort to improve patient safety. However, use of automation and technology is not without risk. Recent literature suggests that automation and technology may cause new types of medication-related errors.1-6
There is little to no published data on which type of technology-related error predominates in healthcare settings where multiple different forms of technology are used. Therefore, the authors conducted an analysis of voluntarily reported medication errors at one institution to determine the following: (1) the quantity of reported medication-related errors associated with the use of technology or automation, (2) the types of technology most likely to be associated with reported medication errors and (3) the stage of the medication use process where reported technology-related errors were most likely to occur (i.e., prescribing, transcription, dispensing, administration, and monitoring).
After IRB approval, data was collected at Advocate Lutheran General Hospital, which is a 645-bed community teaching institution using multiple forms of technology/automation including CPOE, pharmacy information system, smart infusion pumps, automated dispensing cabinets (ADC), pharmacy robot, and an automated inventory management system. Note that at the time of this analysis, bedside point-of-care barcode medication administration had not yet been implemented. At this institution, all healthcare professionals are encouraged to voluntarily report medication errors using an on-line database (MIDAS). The Department of Pharmacy reviews all medication-related events that are reported into this database. All medication-related events submitted electronically into the MIDAS database from January-December 2010 were reviewed to determine if the error was associated with the use of healthcare information technology or automation. If an error was determined by the investigators to be associated with technology or automation, then the specific type of healthcare information technology or automation involved was identified.
Fifty percent (n=351) of all reported medication errors were deemed to be related to the use of technology. In this analysis, CPOE was associated with the largest percentage of reported technology-related errors (31%), followed by the pharmacy information system (20%) (Figure 1). Errors pertaining to patient information (such as allergies, diagnosis, etc.) represented about 11% of the total reported errors. Whereas automation such as ADC or IV pumps represented 9% and 7% of the reported technology related errors, respectively.
Figure 1. The percentage of reported technology-related errors represented by each type of technology is depicted in this pie graph. CPOE = Computerized Prescriber Order Entry, PIS = Pharmacy Information System. ADC = Automated Dispensing Cabinet, eMAR = electronic medication administration record. MED REC = Medication reconciliation.
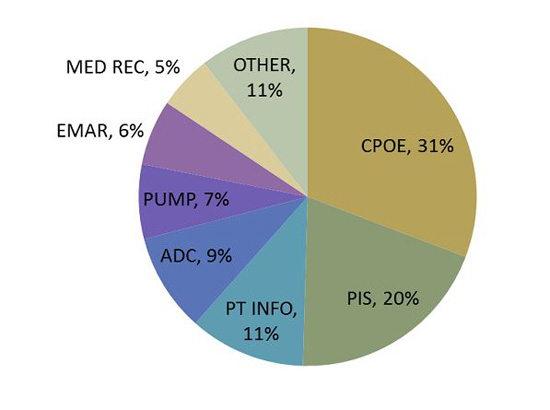
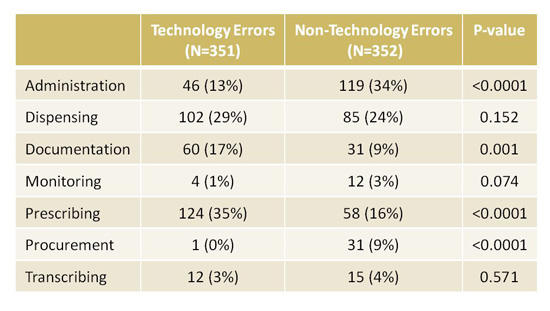
Table 1 depicts the number and percentage of reported technology errors and non-technology errors in each stage of the medication use process. There were more reported technology errors than non-technology errors in the documentation stage [60 (17%) vs. 31 (9%) respectively, p=0.001] and prescribing stage [124 (35%) vs. 58 (16%) respectively, p<0.0001] of the medication use process. This may be explained by the fact that technology (i.e., CPOE, pharmacy information system, or eMAR) is used most commonly in these stages of the medication use process. However, there were more reported non-technology errors than technology errors in the administration stage [46 (13%) vs. 119 (34%), respectively p<0.0001] and procurement stages [1 (0%) vs. 31 (9%) respectively, p<0.0001] of the medication use process. This may be explained by the fact that at Advocate Lutheran General Hospital, bar code scanning for medication administration had not yet been implemented so technology was not being used for this stage of the process at the time of this analysis.
Near misses (errors that did not reach the patient) represented the majority of errors reported. More of the near misses were classified as technology-related errors compared to non-technology-related errors (59% vs. 51%, respectively, p=0.020), which reinforces the protective role that technology may have in preventing errors from actually reaching the patient. There were similar numbers of reported technology and non-technology-related errors that reached the patient and/or caused harm.
Table 1: Technology-related and Non-technology-related Errors by Stage of the Medication use Process Technology Errors
A sub-analysis of this data was conducted to determine trends in medication errors associated specifically with CPOE, since this was the form of technology associated with the most number of errors. One hundred eight records were determined to be related to the use of CPOE. The three most common types of errors were product selection error (24%), dosing error (19%), and incorrect patient error (17%). With regard to the originator of the CPOE order, 84 (78%) were ordered by physicians, of which 61 were entered by residents, 19 by attendings, and 4 were unknown. No one particular physician, physician assistant or nurse had an error rate higher than any other person entering orders. Overall, the top three medications most often involved in CPOE-related errors included electrolytes (11%), enoxaparin (10%) and insulin (9%); all of which are considered high risk medications.
The results of this study were presented at the Medication Safety Subcommittee of the Pharmacy & Therapeutics Committee and shared with Clinical Informatics. The information gained was incorporated into the hospital’s CPOE training program by providing examples of common types of CPOE errors to incoming resident physicians as well as strategies that can be used to prevent them. The training process went smoothly; no barriers were encountered and information provided in the training program was well received. Specific types of CPOE errors and prevention tips were also shared with prescribers via e-mail.
A lesson learned from this analysis is that while technology is intended to improve safety, medication errors will not be eliminated completely and new types of errors may emerge. It is important to continue to collect data on error trends and continually improve processes to reduce the chance for error. It is useful to know which form of technology is the most prone to errors, so that institutions can prioritize safety initiatives centered on that technology. Limitations to this analysis include the fact that this is only one institution’s data and that the data was gathered by analyzing medication error reports, which are voluntary.
REFERENCES
- Miller K, et al. Evaluation of medications removed from automated dispensing machines using the override function leading to multiple system changes. In: Henriksen K, Battles JB, Keyes MA, Grady ML, editors. Advances in Patient Safety: New Directions and Alternative Approaches (Vol. 4: Technology and Medication Safety). Rockville (MD): Agency for Healthcare Research and Quality (US); 2008 Aug.
- Ash JS, et al. The extent and importance of unintended consequences related to computerized provider order entry. J Am Med Inform Assoc. 2007;14:415-23.
- Koppel R, Metlay JP, Cohen A, et al. Role of computerized physician order entry systems in facilitating medication errors. J Am Med Assoc. 2005;293(10):1197-203.
- Rothschild JM, et al. A controlled trial of smart infusion pumps to improve medication safety in critically ill patients. Crit Care Med. 2005;33(3): 533-40.
- Hanuscak TL, et al. Evaluation of causes and frequency of medication errors during information technology downtime. Am J Health Syst Pharm. 2009 Jun 15;66(12):1119-24.
- Borycki E, Keay E. Methods to Assess the Safety of Health Information Systems. Healthcare Quarterly 13 (2010): 47-52.
Board of Pharmacy Update
Highlights from the November Meeting
by Scott A. Meyers, Executive Vice President
The November 12th Board of Pharmacy Meeting was held at the James R. Thompson Center in downtown Chicago. These are the highlights of that meeting.
Board elections – The first order of business for the Board was election of officers for the 2014 calendar year. Phil Burgess was re-elected as chair by common consent. Miriam Mobley-Smith was elected Vice Chair in a secret ballot over Ned Milenkovich.
Practice Act Rules Progress – A second draft of the Pharmacy Practice Act Rules revision has been distributed to the professional organizations and other key pharmacy stakeholders for review and comment. Department staff hopes to have a third and final draft ready for review by the Governor’s office by the end of the month and anticipates publishing that draft with any revisions recommended by the Governor in an early January 2014 Illinois Register.
Publication of draft rules in the Illinois Register initiates a 45-day public comment period, which at its conclusion, the Department staff will respond to all comments and incorporate changes that are considered appropriate based on those comments. The final draft of the rules will then be sent to the Joint Committee on Administrative Rules (4 Senators, 4 Representatives representing both parties equally) for final approval.
The process is anticipated to be complete sometime in the spring. The current revision of the rules is available on the members’ only section of the ICHP website on the Public Policy Page.
Student Pharmacist Registration – This year’s registration renewals for pharmacy technicians, certified pharmacy technicians and student pharmacists was fraught with issues again, primarily concerning student pharmacist registrations. Miriam Mobley-Smith will work with all the colleges to coordinate next year’s efforts and to be a conduit to the Department. Pharmacy directors who send in e-batch renewals are cautioned and urged to identify any of their pharmacy technicians who may be, at the time of renewal, enrolled in a College of Pharmacy and not renew those technician registrations without consulting the students. Pharmacy directors and managers and chain pharmacy administrators have complicated the process for many students over the past couple of years by using the e-batch renewal process.
NABP/AACP District IV Meeting Report – The Illinois Board of Pharmacy and Chicago State University College of Pharmacy hosted the 80th Annual Meeting of NABP’s District IV in Alsip, on November 6-8. The meeting set all-time records for attendance and for fund raising. Programming focused on the theme “Navigating Health Care Reform Opportunities: Enabling Pharmacists to Practice at the Top of Their Profession”. Educational sessions focused on the Affordable Care Act, Biosimilars, Indigent Care, and Collaborative Practice. In addition, members of NABP present at the meeting voted to support resolutions from other districts that will be debated at the 2014 NABP Annual Meeting next May. The resolutions focused on the following issues:
- Educating patients on the pitfalls of obtaining medications from sources outside the US
- Developing standards for use of data collected by state prescription drug monitoring programs
- Including veterinary medications in college of pharmacy curriculums
Change in Future Board Meeting Times – The Board was asked by Department staff if they would be amenable to changing the Board of Pharmacy meeting times from the usual 9:30 AM to one hour later or 10:30 AM retaining the current second Tuesday of odd months for the meetings. The Board felt this would not create any hardship and accepted the change beginning with the January 14, 2014 meeting.
Legislative Update – Scott Meyers, ICHP Executive Vice President, provided a very brief legislative update to the Board of Pharmacy. No action related to pharmacy issues occurred during the veto session. Next spring’s session is expected to see continued pressure for a biosimilars bill and efforts by ICHP and IPhA may include creation of a provider status bill, adding the requirement for CE for Certified Pharmacy Technicians, standardized audit rules of PBM and other insurance audits, and MAC (Maximum Allowable Cost) transparency with the Department of Healthcare and Family Services.
Open Forum – The Board entertained issues from those present in the audience during this part of the meeting. Garth Reynolds, Executive Director of the Illinois Pharmacists Association, provided the Board members and attendees with an article from North Carolina criticizing their Board of Pharmacy for not meeting pharmacy inspection goals for several years. Mr. Reynolds encouraged the Board and the Department to step up regular inspections of Illinois pharmacies to prevent this type of press from appearing here. The Board agreed and voted to require all pharmacies to complete and retain an annual self-inspection form currently available on the IDFPR website beginning in 2014. The inspection form must be accurate and available for any inspector. Currently the self-inspection form pertains to community pharmacy practice. ICHP will provide input to the Department to develop a hospital self-inspection form in the coming months.
Next Board of Pharmacy Meeting – Is scheduled for Tuesday, January 14 at 10:30 AM on the 9th floor of the James R. Thompson Center in downtown Chicago. Pharmacists, pharmacy students and pharmacy technicians are welcome to attend the open portion of the meeting.
New Practitioners Network
How to Get The Most Out of Your Residency Showcase Experience
by Alex Keppel, Pharm. D.
This time of year is always highly anticipated in pharmacy circles as ASHP’s Midyear Clinical Meeting is approaching. Last year I was fortunate enough to be able to attend my first one, as both a student presenting a poster and as a student looking to learn more about residency programs.
One of the many highlights of the Midyear Clinical Meeting is the Residency Showcase, aimed at students or practitioners seeking a residency position. The opening to the showcase is quite an awe-inspiring sight in itself; hundreds upon hundreds of students from all over the country packed like sardines outside the conference hall, waiting for the doors to open and the showcase to begin. And once the doors open it’s a free-for-all for the next three hours as everyone tries to ask their questions and get their face-time with any number of different programs. As an attendee, it’s easy to get caught up in this moment and lose sight of why you’re there or what you’re hoping to get out of it.
It’s likely that those 3 hours are the only chance you’ll get to talk to the residents, preceptors, or directors about what their program offers and have them specifically address any questions or concerns you may have outside of the actual interview. So with that in mind, I’d like to give a few tips for any of you planning to attend this year so that you can truly maximize your time in the showcase and hopefully walk away with your questions answered and a good idea of the programs you’ll be applying to. Let’s get started:
Tip 1: Make a list, check it twice. It is important to have a list of the programs you want to look at before those doors open. If you haven’t looked at the schedule, you may be surprised to learn that there are 3 different time slots dedicated to the residency showcase. Furthermore, all programs are only at one of the sessions. So it is important to know who you want to look at so you can be sure to go to their session.
Tip 2: Plan your route. Along with the schedule, there is a map of each session and the location of each program’s booth. USE THIS TO YOUR ADVANTAGE! Look at the map, find the programs you’re interested in and plot the best way to get to each of them. I cannot stress how helpful it is to have a route planned beforehand because nothing will waste more time than aimlessly walking around trying to figure out where a program’s booth is set up, especially when you consider the crowd of people you’ll be squeezing through to get there.
Tip 3: Be flexible and open-minded. Now just because you took my advice and made your list of programs and planned your route ahead of time, doesn’t mean it will all go as planned. Remember, there are only so many people representing each program and when you reach them it may be the same time that crowds of others get to them as well. So what now? Don’t waste time standing and waiting, look around at surrounding booths and if they are less crowded, go talk to them. You may end up discovering that you really like their program, but if nothing else, you can keep an eye on your desired stop and when the crowd thins you’re not far away.
Tip 4: Don’t wait until the showcase to learn about your program. Many programs have websites that cover in detail what their goals are. Check these out before you get to the showcase so that you can answer some of your more generic questions beforehand. That way you can talk more deeply with the program representatives and find out specifically about the program and how it will fit your needs. Before application deadlines you want to be sure that the program is a good fit for you and your goals as a budding practitioner, and you will have more time to find this out at the showcase if other questions are already answered.
Tip 5: Prepare questions for them. This goes hand in hand with Tip 4. By getting your general questions answered with your research on the program, you’ll then have time to ask them more pointed questions about what you’re looking for from them. Do they hire a lot of former residents? Do they emphasize teaching? Do they have elective rotations that possibly weren’t listed on their website or brochure? Are they flexible in developing rotations to fit the resident’s desires? Whatever the case may be, these types of questions are helpful for multiple reasons. Not only do you gain answers specific to you, but also these help you stand out in their mind. With the hundreds of people passing through, they end up giving the same answers over and over. With your more personal and specific questions, you open the door for a conversation that they may recall when your application crosses their desk and they are selecting people for interviews.
Tip 6: Relax, have fun, smile. This is the first impression most programs are getting of you, so do you want that impression to be of a nervous, stressed out, unhappy person? Of course not, you want them to remember how calm and cool you were. So relax and give them a good smile; remember this is mostly about you choosing them for your applications. Your moment in the hot seat will come at the interviews, but right now you’re the one making the choices, not them, so there’s no pressure!
Tip 7: DON’T BE SHY! Of all the times to be shy and quiet, this is definitely not one. For many of you, this may be your first interaction with pharmacists other than professors, preceptors, or fellow students and if so, you will learn very quickly how important networking is. Networking is the difference between having your foot in the door or being on the outside looking in. So dive right in, meet people, and talk! Learn about them and let them learn a little about you, be it personal or professional. Who knows, you may even come out the other side with new friends! But you’re definitely not going to get ANYTHING out of the showcase if you go into it with a shy, quiet attitude.
Looking back at last year, I don’t understand why I was so nervous and anxious going into the showcase, so hopefully these tips will help calm any of those nerves you may be having. The entire week was really fun and the showcase was nowhere near the stress level I built it up to be. So to reemphasize Tip 6, you’re on vacation, so HAVE FUN and enjoy every minute because the week goes fast and you’ll be heading back home before you know it.
The GAS From Springfield
Provider Status in Illinois?
by Jim Owen and Scott Meyers
California has now joined New Mexico and North Carolina in passing a bill that allows pharmacists (some, not all) to practice closer to the top of their training. Senate Bill 493 passed the California Assembly and was promptly signed by Governor Jerry Brown on October 1st. This bill allows “Advanced Practice Pharmacists” (APPs) to initiate nicotine replacement therapy, oral contraceptives and some immunizations without a prescription or collaborative agreement. In addition, the APPs may order labs, administer drugs and biologicals that have been ordered by a prescriber, and initiate, modify or discontinue medications under a collaborative agreement with a physician.
To be licensed as an “Advanced Practice Pharmacist” in California, you must meet all of the following criteria:
- Hold an active license to practice pharmacy that is in good standing,
- Satisfy any two of the following criteria:
- Earn a certification in a relevant area of practice, including but not limited to, ambulatory care, critical care, geriatric pharmacy, nuclear pharmacy, nutritional support pharmacy, oncology pharmacy, pediatric pharmacy, pharmacotherapy, or psychiatric pharmacy from an organization recognized by the Accreditation Council on Pharmacy Education or another entity recognized by the board.
- Complete a postgraduate residency through an accredited postgraduate institution where at least 50 percent of the experience includes provision of direct patient care services with interdisciplinary teams.
- Have provided clinical services to patients for at least one year under a collaborative practice agreement or protocol with a physician, advance practice pharmacist, pharmacist practicing collaborative drug therapy management, or health system.
- File an application with the board for recognition as an advanced practice pharmacist.
- Pay the applicable fee to the board.
You can see, this great step forward is not open to all pharmacists. And that’s probably what will happen federally and in most other states. In New Mexico and North Carolina, there are additional requirements to become a “pharmacist clinician” or “clinical pharmacist practitioner” respectively.
So what’s the plan for Illinois? The first step will be to see where our members stand. That, by itself, may not determine the tract we take once we move forward. We will then need to speak with the other key players in Illinois Pharmacy, the Illinois Pharmacists Association (IPhA) and the Illinois Retail Merchants Association (IRMA). If the three of us can’t get together and agree on a plan, it is extremely difficult, okay, let’s say impossible, to get anything passed by the General Assembly. If we all agree, the battle is far from over. The Illinois State Medical Society is a formidable foe and they must be convinced that this will not cut into their piece of the healthcare financing pie. It’s going to be a hard fight but by suggesting that an APP would be a physician extender, there may be hope. And truly that’s what the APPs will be.
Once the physicians are on board, then it’s the PAs and probably more importantly the APNs. They’ll fight this tooth and nail because when it comes to medication therapy management, they know we would have the upper hand and could definitely cut into their piece of the pie.
The good news is that predictions call for a significant primary care provider shortage within the next five years, and this model will go a long way to minimize that shortage by extending the patient load the PCPs can handle.
So gird your loins for a tough fight, assuming pharmacy can get its own house in order, as we hopefully begin to tackle “provider status” in Illinois. It won’t hurt that the fight will also be taking place federally, hopefully after the first of the year.
Another legislative initiative ICHP hopes to launch, is the establishment of mandatory CE hours for certified pharmacy technicians. While this might not make some of our technician members happy, ICHP now provides 20 hours of online CE for member technicians completely free! Pharmacy Tech Topics™, ICHP’s home-study CE product has provided certified technicians with all the CE they need for PTCB recertification and beginning this fall this $45 a year subscription is available free for ICHP member techs. And ICHP has no desire to ask the State to require more hours of CE than PTCB does.
2014 will be an interesting legislative year regardless of the pharmacy legislation. It looks like pension reform will still be on the agenda along with projected tax increases and who knows what else. Now it is more important than ever to be an informed and engaged member of ICHP. Whether you support provider status or mandatory CE for certified pharmacy technicians, we’ll provide you with timely updates and recommend important actions to take. These legislative battles can’t be won with a handful of lobbyists and experts, they take grassroots support from people directly affected by the proposed changes.
Keep watching for more information via email and in future issues of the “GAS”!
ICHPeople
Please welcome newly elected ICHP officers
Linda Fred – President-elect
Charlene Hope – Secretary-elect
Mike Weaver – Chair of the House
Kathryn Schultz – Director-elect, Government Affairs
Travis Hunerdosse – Director-elect, Educational Affairs
Carrie Vogler – Director-elect, Marketing Affairs
Brandi Strader – Chair-elect, New Practitioners Network
Ana Fernandez – Technician Representative-elect
College Connections
Keys to Successfully Completing Research: A Student’s Perspective on the Mentor/Mentee Relationship
by Mital K. Patel, P-4, and Sweta K. Patel, P-4, Chicago State University College of Pharmacy
Have you ever done research before? If not, do you think you may be interested? Our personal research experience will give both potential students and mentors an insider’s perspective…read on to learn more!
The Chicago State University College of Pharmacy’s (CSU-COP) Capstone Research Program is one of the requirements a fourth year professional student must undergo for graduation. The requirement consists of a yearlong research project that students develop and implement under the guidance of a mentor, with final culmination resulting in a research manuscript and poster suitable for publication/formal poster presentation. In our opinion, the program is immensely beneficial for all students regardless of their interest in pursuing a career focused on research. From a mentor’s standpoint, students can help in accomplishing many research-related tasks including performing a literature search, obtaining institutional review board (IRB) approval, collecting data, and developing a research manuscript.
During the Summer of 2013, we had the opportunity to work with Dr. Rosalyn P. Vellurattil on a capstone research project assessing pharmacy students’ perceptions of a mock research project in preparation for a fourth year research requirement utilizing a survey for our method of data collection. To begin our research project, we completed preliminary steps including performing a literature search, writing a research proposal, obtaining IRB approval, and developing a survey instrument. From the very beginning, we received continuous guidance and feedback. Frequent communication between us and Dr. Vellurattil was essential in order to develop the research project. The way our mentor kept us on track was by providing us with a calendar of deadlines for each research task we needed to complete. We found it beneficial to complete each draft ahead of the deadline so we could have more time for feedback and reconstructing it. It also made it easier for our mentor because she did not have to wait until the last moment to review our work.
After developing the survey instrument, we pilot-tested the survey on our peers. What a great experience! Our peers’ feedback was really helpful in evaluating the competency of the questionnaire and estimating the time it took to take the survey. More exciting parts of our project are yet to come, including administering the survey, collecting and analyzing the data, creating a poster presentation, and developing the manuscript.
In addition to learning about our research topic, we learned to work independently, evaluate scientific literature, improve oral and written communication, and enhance problem-solving and critical thinking skills. Because of our mentor’s constant encouragement and good time management, we were able to perform other activities in addition to research, including creating supplemental handouts for fourth year students and writing reflections about our own research experience.
So, you may now be thinking...what about the mentor? A research experience is not only rewarding for the mentee, but can also be satisfying for mentors.1,2 Let us dispel some common myths regarding research mentoring:
MYTH: “Mentors are busy or have many competing responsibilities. Having students inevitably decreases productivity.”
FACT: Studies have shown that students may actually increase productivity.1,2 Students can aid mentors by decreasing some of the workload they would be doing if they were conducting the research on their own, which can lead to more time to manage other responsibilities.
MYTH: “Only CSU-COP faculty can be a part of the Capstone Research Program.”
FACT: Anyone who is interested in research can be involved with the experience! Faculty, preceptors, employers, pharmacists and any other interested parties can be a capstone mentor. Research projects include, but are not limited to, laboratory research, clinical research, educational research, business plan development, public health and drug utilization review. Click on the following link for more information: http://www.csu.edu/pharmacy/capstoneexperience.htm
MYTH: “A six week APPE module is mandatory for the CSU-COP capstone research project.”
FACT: Mentors may or may not require students to take a six week APPE module with them. Mentors who require APPE modules can choose any module based on their availability. If this is not preferred, students and mentors can communicate how they will approach the project for the year.
MYTH: “I can’t be a mentor because I don’t have any research where I practice.”
FACT: Anything you do can be turned into research - from patient satisfaction, to drug utilization review, outcomes of services you provide, or hospital/community initiatives. Just think about what you are doing right now or what you would like to do, and how you can potentially assess it. The possibilities are endless!
MYTH: “Mentors don’t have time for students.”
FACT: Mentors help facilitate and guide a pharmacy student throughout their research experience. The relationship is built on trust and respect. If you go into the experience with an open-mind and dedication to your work, your mentor will make time for you.
Our capstone research project has been an invaluable experience thus far. It has awakened an interest in further research in the future for us. From our experience, research keeps you up-to-date on not only what is current in pharmacy, but also on what gaps exist, and what the future may hold. Having research experience strengthens your skills in providing quality pharmaceutical care, and the valuable relationship you build with your mentor is rewarding both personally and professionally. Performing research allows students a chance to place their knowledge learned in the classroom into a real world environment. Whether you’re a student interested in research, or a researcher interested in mentoring, we encourage you to get involved today!
References:
1. Kiersma ME, Hagemeier N, Chen AM, et al. A graduate student mentoring program to develop interest in research. Am J Pharm Educ. 2012;76(6):Article 104.
2. Wuller C. A capstone advanced pharmacy practice experience in research. Am J Pharm Educ. 2010;74(10):Article 180.
Keep Your Eyes and Ears Open
by Cheyenne Newsome, P-4, Southern Illinois University Edwardsville School of Pharmacy
There are amazing opportunities for professional growth available if you keep your eyes and ears open. By participating in outside activities during my time in pharmacy school, I have gained skills, insights, and confidence that truly cannot be learned in a classroom.
Many pharmacy students spend hours in a community pharmacy providing care to patients, not realizing all the knowledge they are collecting. Working in this environment develops counseling skills through patient interaction and increases familiarity with drugs. I was able to answer many questions my preceptors posed during rotations because of my community interactions. At times, working with a ‘floater’ pharmacist is viewed by pharmacy intern as a hardship. Instead, keep your eyes and ears open and view it as an opportunity to observe different counseling styles and gain other perspectives on how to practice pharmacy. Additionally, the conversations with patients, insurance companies, supervising pharmacists and managers teach strategies to problem solve that are not found in textbooks or lectures.
Although working part time assures you frequent pharmacy interactions, less obvious opportunities can prove invaluable. Participating in Student Society of Health System Pharmacists (SSHP) events is another great way to gain experience and improve patient care skills while also serving your community. SSHP’s ‘This Side of the Dirt’ presentations allow pharmacy students to provide medication abuse education to junior high students. Developing public speaking skills, gaining insight into effectively communicating with various age groups, and learning about drug abuse are all tangential benefits of participating in professional organizations. Experiences like this improve confidence in facilitating topic discussions on Advanced Pharmacy Practice Experiences (APPEs). There are many benefits to be gained from participating in your chapter activities for all involved. Listen closely at chapter meetings for opportunities of interest to you.
Shadowing practicing pharmacists, either those on your faculty or those in an area of interest to you, provides information, networking and skill sets that can lead to helping you define your desired area of practice in the field of pharmacy. If you are shadowing faculty members, you will find diverse specialties and the possibility of creating professional relationships with your faculty members. This experience can also provide insight on career paths that faculty have followed and an opportunity to extract advice to help you on your path, and potentially gain a mentor. It may seem strange, but in a few short years, faculty will no longer be your superiors, but your peers. Pharmacy is a small world, and taking the time out from your studies to spend time watching and listening to successful pharmacists can open many doors.
As students, we are provided with many open doors and opportunities. Dedicate some time to engage in experiences outside of the classroom. Benefits to doing so include identifying areas of pharmacy that interest you, discovering where you want to take your pharmacy career, advancing your patient care skills, and improving professional confidence. In every professional experience you choose, keep your eyes and ears open. You might be surprised by what you discover.
Professional Practice Makes Perfect
by Sarah Cotner (P3) – University of Illinois at Chicago
As the Professional Practice Chair of our student chapter, I had the opportunity to organize the preliminary round of the ASHP Clinical Skills Competition at the University of Illinois at Chicago. Our local competition took place on Wednesday, October 16th. For those unfamiliar with the Clinical Skills Competition (CSC), the purpose is to encourage and recognize excellence in clinical skill development for pharmacy students. The CSC is designed to facilitate an interactive, team-based analysis of clinical scenarios for health-system pharmacists (and pharmacy students) to help patients make the best use of their medications. During the competition, students work on a timed case study in pairs. Teams have 2 hours to complete the following tasks: assess patient information and current therapy, identify drug therapy problems, and develop a pharmacist's care plan. Each team is required to give a 2-minute oral presentation justifying their care plan recommendation for the patient’s most urgent problem. This is followed by an 8 minute question and answer session. A panel of judges determines the winner of the competition using a standardized set of evaluation criteria. The team with the highest combined score of the written assessment and oral presentation is declared the winner. Preliminary round winners receive complimentary registration to the 48th ASHP Midyear Clinical Meeting in Orlando, FL in December.
Due to the time required to compete, registration was limited to 10 teams and open to students on a first come, first serve basis. Registration priority was given to P4s initially, and the following day registration was going to open up to P3s. In the past, half the teams have consisted of P4 students and the remaining teams have consisted of P3 students. This year, all slots were filled by P4s from both the Chicago and Rockford campuses within one minute of opening registration!
There is no doubt that the clinical responsibilities of pharmacists are growing. In turn, the interest in clinical skill development among students is on the rise. Events such as the Clinical Skills Competition allow students to “practice clinical practice”. Since being elected Professional Practice Chair, I have often interpreted the definition of practice to be the exercise, performance, or application of a profession. Another definition of practice is the action of doing something again and again in order to get better at it. Coming from undergrad with the background of a student athlete, I understand that this type of practice cannot be overlooked. Students involved with ICHP and ASHP have numerous opportunities to practice their future practice. To be the best of the best, extra preparation outside of school is needed before the making it to the big leagues.
On October 16th, CSC participants competed in front of an all-star panel of judges, Drs. Mary Moody, Lara Ellinger, and Charles McPherson. These faculty members coach students in and outside of the classroom at UIC. Their willingness help students learn by doing is truly appreciated.
After much deliberation, the winning team was chosen. Good luck to Lori McGuire and Stephanie Dwyer at the national competition in Florida! Remember, professional practice makes perfect.
More
Officers and Board of Directors
TOM WESTERKAMP Immediate Past President224-948-1528 tom_westerkamp@baxter.com
LINDA FRED
President-Elect
217-383-3253 linda.fred@carle.com
GINGER ERTEL Treasurer 660-342-5022 gertel@msn.com CAROL HEUNISCH Secretary 847-933-6811 cheunisch@northshore.orgTRAVIS HUNERDOSSE Director, Educational Affairs Travis_Hunerdosse@rush.edu
JENNIFER ELLISON Director, Marketing AffairsJennifer.C.Ellison@osfhealthcare.org
DESI KOTIS Director, Professional Affairs
JENNIFER PHILLIPS Assistant Editor, KeePosted 630-515-7167 jphillips@midwestern.edu KATHRYN SCHULTZ Regional Director North
JULIE BUCEK Student Chapter LiaisonUniversity of IL C.O.P. bucek@uic.eduNADIYAH CHAUDHARY President, Rockford Student Chapter University of IL C.O.P. nadi925@gmail.comJANEY YU President, Student ChapterMidwestern University C.O.P. janey.yu@mwumail.midwestern.edu
BERNICE MAN President, Student Chapter Chicago State University C.O.P. bman@csu.edu TRAMAINE HARDIMON Student Representative Chicago State University C.O.P thardimo@csu.edu ZAK VINSON President, Student Chapter Southern Illinois University S.O.Pzvinson@siue.edu
ALEX MERSCH President, Student Chapter Roosevelt University C.O.P. amersch@mail.roosevelt.edu
JENNIFER AGUADO President, Student Chapter Rosalind Franklin University C.O.P. jennifer.aguado@my.rfums.org SCOTT MEYERS Executive Vice President, ICHP Office 815-227-9292 scottm@ichpnet.org
ICHP AFFILIATES
PETE ANTONOPOULOS President, Northern IL Society (NISHP) JULIA SCHIMMELPFENNIG President, Metro East Society (MESHP) jschimmelpfen@sebh.org MEGAN METZKE President, Sangamiss Society memiller8@yahoo.com
ED RAINVILLE President, West Central Society (WSHP) 309-655-7331x ed.c.rainville@osfhealthcare.org
Vacant Roles at Affiliates —
Director, Government Affairs; President, Rock Valley Society; Southern IL Society; Sugar Creek Society
Welcome New Members!

| New Member |
Recruiter |
| Billee John |
Anna Arthur |
| Christine Ciaramella |
|
| Danielle Magas |
|
| Jeril George |
|
| Tania John |
|
| Alexander Keppel |
Diana Isaacs |
| Katrina Karpowitsch |
|
| Elizabeth Van Dril |
|
| Megan Wesling |
|
| Marisela Luciano |
|
| Nicole Argus |
|
| Dawniesha Willis |
|
| Majlinda Dervishi |
|
| Chris Steinwender |
|
ICHP Pharmacy Action Fund (PAC) Contributors
Names below reflect donations between December 1, 2012 and November 30, 2013. Giving categories reflect each person's cumulative donations since inception.
GENERAL ASSEMBLY GUILD - $1000 & More Scott BergmanKevin ColganEdward DonnellyDave HicksFrank KokaislWilliam McEvoy
Scott Meyers
Michael Novario
Michael Weaver
Thomas Westerkamp
SPRINGFIELD SOCIETY - $500-$999 Stephanie CrawfordRauf Dalal
CAPITOL CLUB - $250-$499
Margaret Allen
Vern Johnson
Janette Mark
Edward Rainville
Heidi Sunday
Jill Warszalek
LINCOLN LEAGUE - $100-$249
Anonymous
Marie Williams
GRASSROOTS GANG - $50-$99
Jennifer Ellison
Tory Gunderson
Glenna Hargreaves
CONTRIBUTOR - $1-$49 John Chaney
Izabela Wozniak
Upcoming Events

Tuesday, December 3
Non-CPE NISHP Program: Effient (prasugrel): Antiplatelet Therapy for Patients with Acute Coronary Syndrome (ACS) Managed with Percutaneous Coronary Intervention (PCI)
Maggiano's | Oakbrook, IL
Tuesday, December 9
Illinois Reception at Midyear
Rozen PLAZA Hotel across from Pointe Orlando | Orlando, FL
_web578x100.png)
Print Entire Issue